

Pre-transplant immune profile defined by principal component analysis predicts acute rejection after kidney transplantation
- PMID: 37497224
- PMCID: PMC10367005
- DOI: 10.3389/fimmu.2023.1192440
Pre-transplant immune profile defined by principal component analysis predicts acute rejection after kidney transplantation
Abstract
Background: Acute rejection persists as a frequent complication after kidney transplantation. Defining an at-risk immune profile would allow better preventive approaches.
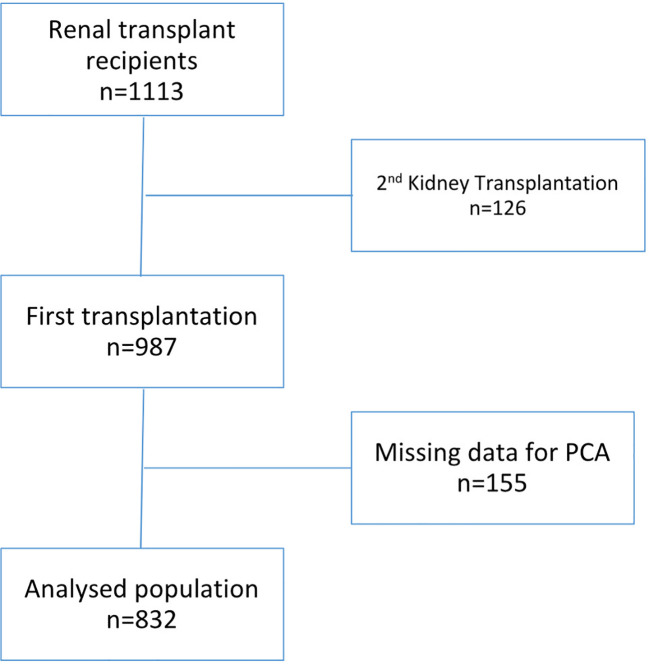
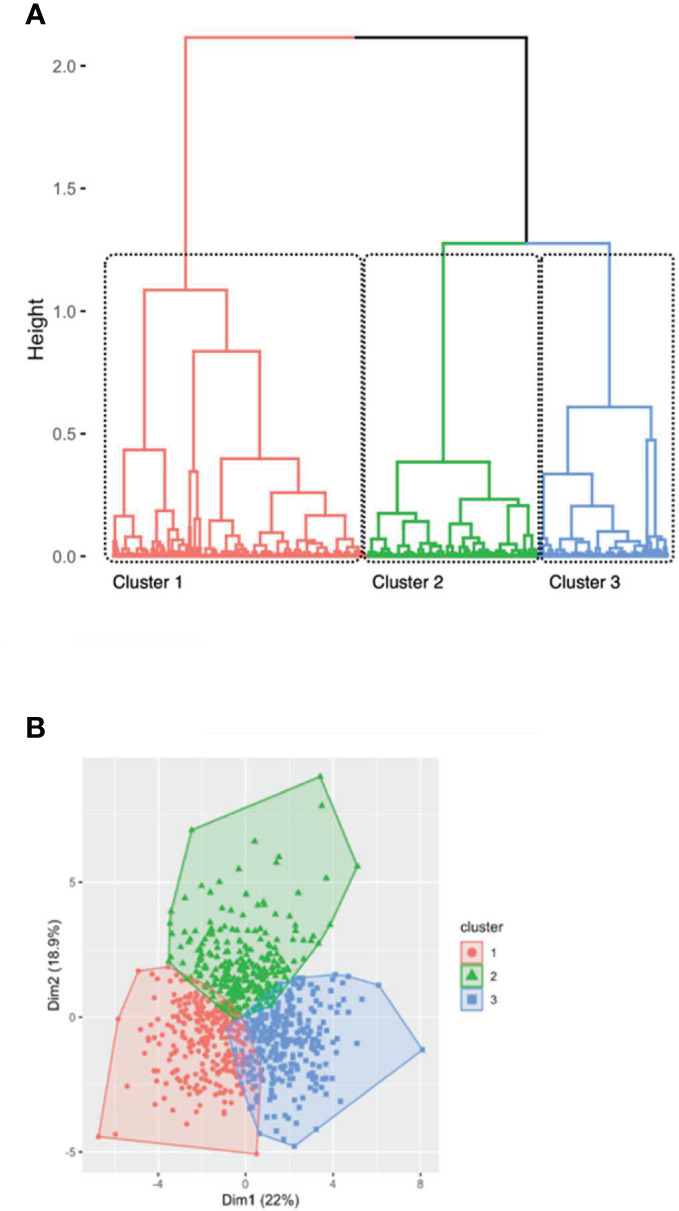
Methods: We performed unsupervised hierarchical clustering analysis on pre-transplant immunological phenotype in 1113 renal transplant recipients from the ORLY-EST cohort.
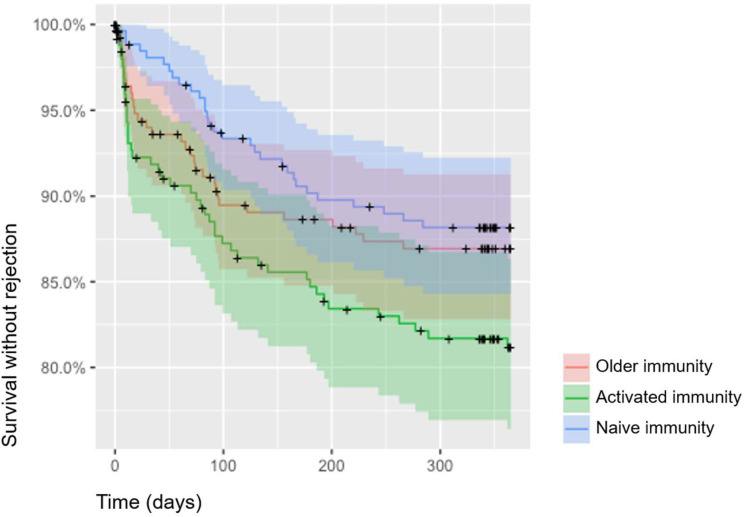
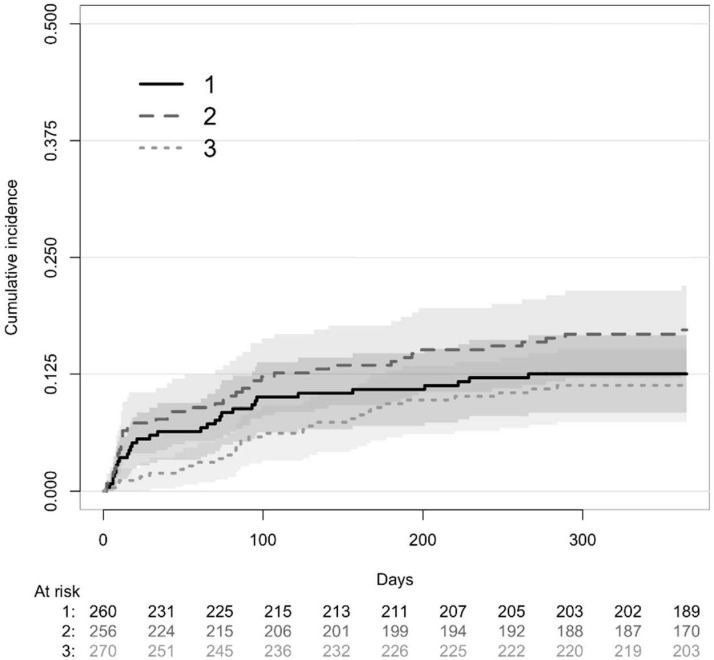
Results: We identified three immune profiles correlated with clinical phenotypes. A memory immune cluster was defined by memory CD4+T cell expansion and decreased naïve CD4+T cell. An activated immune cluster was characterized by an increase in CD8+T cells and a decreased CD4/CD8 ratio. A naïve immune cluster was mainly defined by increased naïve CD4+T cells. Patients from the memory immune profile tend to be older and to have diabetes whereas those from the activated immune profile were younger and more likely to have pre-transplant exposure to CMV. Patients from the activated immune profile were more prone to experience acute rejection than those from other clusters [(HR=1.69, 95%IC[1.05-2.70], p=0.030) and (HR=1.85; 95%IC[1.16-3.00], p=0.011). In the activated immune profile, those without previous exposure to CMV (24%) were at very high risk of acute rejection (27 vs 16%, HR=1.85; 95%IC[1.04-3.33], p=0.039).
Conclusion: Immune profile determination based on principal component analysis defines clinically different sub-groups and discriminate a population at high-risk of acute rejection.
Keywords: acute rejection; biomarker; hierarchical clustering analysis; immune profile; kidney transplantation.
Copyright © 2023 Gaiffe, Colladant, Desmaret, Bamoulid, Leroux, Laheurte, Brouard, Giral, Saas, Courivaud, Degauque and Ducloux.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials