

Validation of Immunotherapy Response Score as Predictive of Pan-solid Tumor Anti-PD-1/PD-L1 Benefit
- PMID: 37497337
- PMCID: PMC10367935
- DOI: 10.1158/2767-9764.CRC-23-0036
Validation of Immunotherapy Response Score as Predictive of Pan-solid Tumor Anti-PD-1/PD-L1 Benefit
Abstract
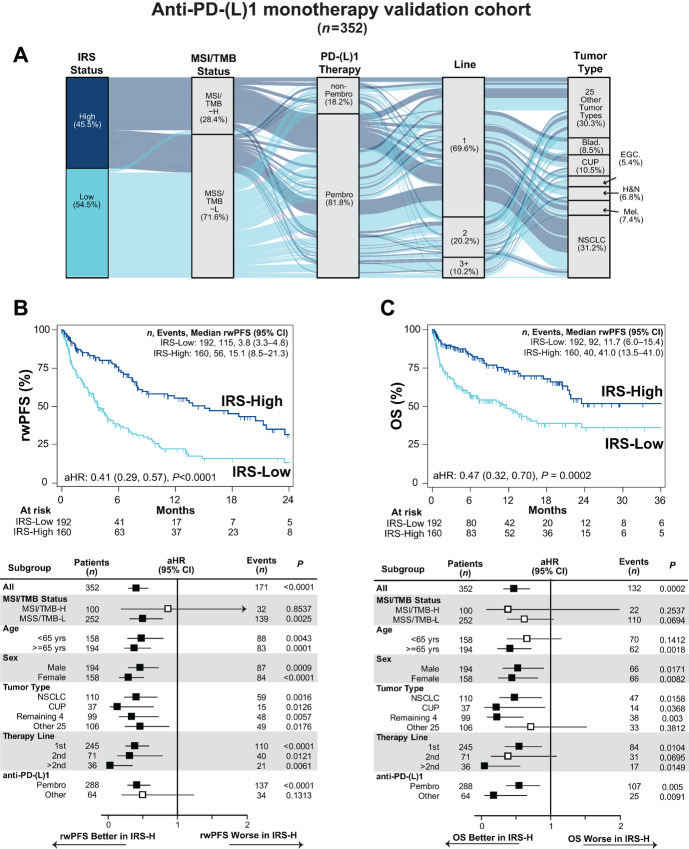
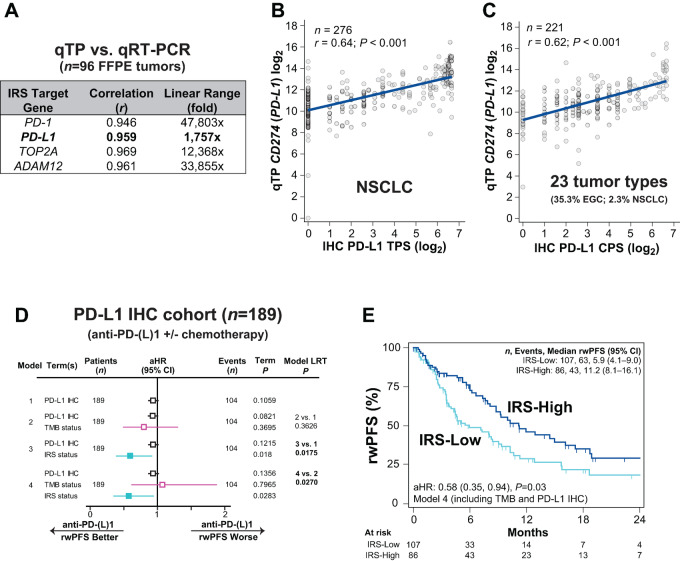
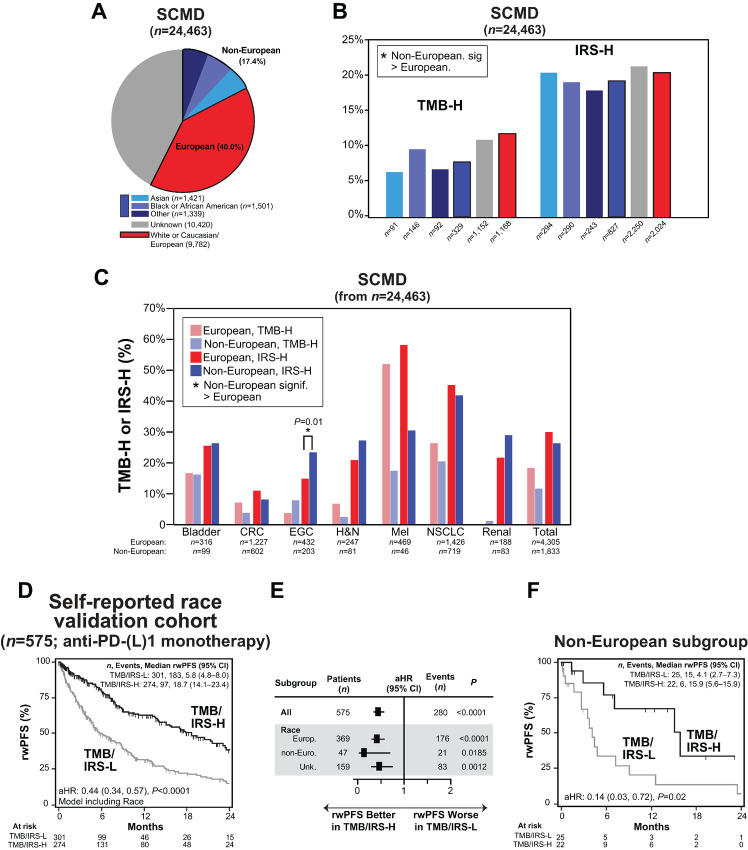
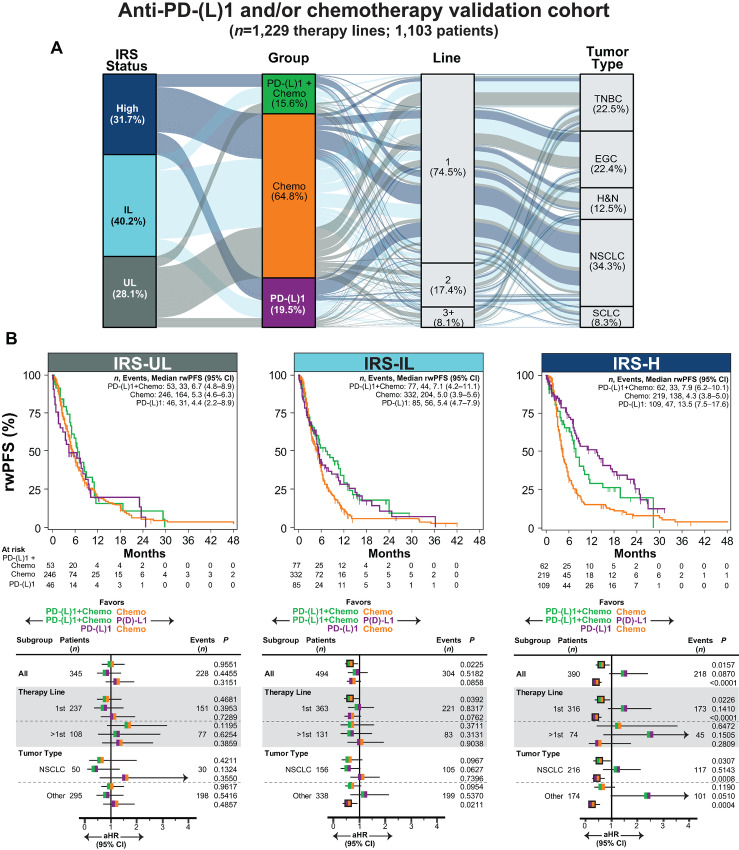
Immunotherapy response score (IRS) integrates tumor mutation burden (TMB) and quantitative expression biomarkers to predict anti-PD-1/PD-L1 [PD-(L)1] monotherapy benefit. Here, we evaluated IRS in additional cohorts. Patients from an observational trial (NCT03061305) treated with anti-PD-(L)1 monotherapy were included and assigned to IRS-High (-H) versus -Low (-L) groups. Associations with real-world progression-free survival (rwPFS) and overall survival (OS) were determined by Cox proportional hazards (CPH) modeling. Those with available PD-L1 IHC treated with anti-PD-(L)1 with or without chemotherapy were separately assessed. Patients treated with PD-(L)1 and/or chemotherapy (five relevant tumor types) were assigned to three IRS groups [IRS-L divided into IRS-Ultra-Low (-UL) and Intermediate-Low (-IL), and similarly assessed]. In the 352 patient anti-PD-(L)1 monotherapy validation cohort (31 tumor types), IRS-H versus IRS-L patients had significantly longer rwPFS and OS. IRS significantly improved CPH associations with rwPFS and OS beyond microsatellite instability (MSI)/TMB alone. In a 189 patient (10 tumor types) PD-L1 IHC comparison cohort, IRS, but not PD-L1 IHC nor TMB, was significantly associated with anti-PD-L1 rwPFS. In a 1,103-patient cohort (from five relevant tumor types), rwPFS did not significantly differ in IRS-UL patients treated with chemotherapy versus chemotherapy plus anti-PD-(L)1, nor in IRS-H patients treated with anti-PD-(L)1 versus anti-PD-(L)1 + chemotherapy. IRS associations were consistent across subgroups, including both Europeans and non-Europeans. These results confirm the utility of IRS utility for predicting pan-solid tumor PD-(L)1 monotherapy benefit beyond available biomarkers and demonstrate utility for informing on anti-PD-(L)1 and/or chemotherapy treatment.
Significance: This study confirms the utility of the integrative IRS biomarker for predicting anti-PD-L1/PD-1 benefit. IRS significantly improved upon currently available biomarkers, including PD-L1 IHC, TMB, and MSI status. Additional utility for informing on chemotherapy, anti-PD-L1/PD-1, and anti-PD-L1/PD-1 plus chemotherapy treatments decisions is shown.
© 2023 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Sharma P, Siddiqui BA, Anandhan S, Yadav SS, Subudhi SK, Gao J, et al. The next decade of immune checkpoint therapy. Cancer Discov 2021;11:838–57. - PubMed
-
- Marabelle A, Fakih M, Lopez J, Shah M, Shapira-Frommer R, Nakagawa K, et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol 2020;21:1353–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
