

Stoma-free Survival After Rectal Cancer Resection With Anastomotic Leakage: Development and Validation of a Prediction Model in a Large International Cohort
- PMID: 37498208
- PMCID: PMC10549897
- DOI: 10.1097/SLA.0000000000006043
Stoma-free Survival After Rectal Cancer Resection With Anastomotic Leakage: Development and Validation of a Prediction Model in a Large International Cohort
Abstract
Objective: To develop and validate a prediction model (STOMA score) for 1-year stoma-free survival in patients with rectal cancer (RC) with anastomotic leakage (AL).
Background: AL after RC resection often results in a permanent stoma.
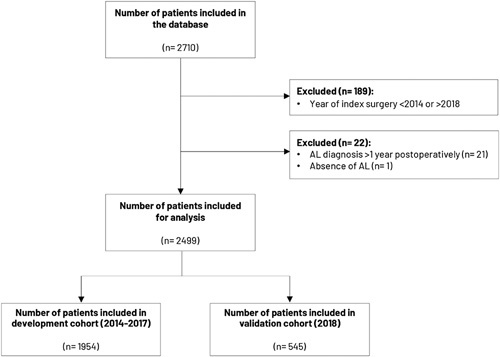
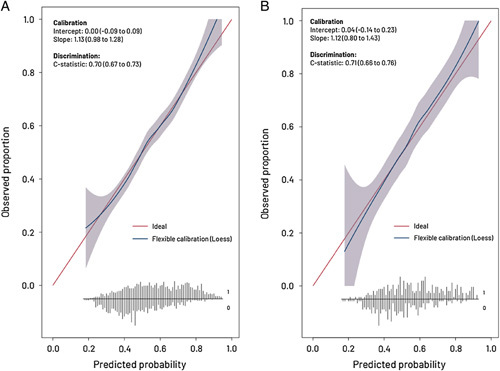
Methods: This international retrospective cohort study (TENTACLE-Rectum) encompassed 216 participating centres and included patients who developed AL after RC surgery between 2014 and 2018. Clinically relevant predictors for 1-year stoma-free survival were included in uni and multivariable logistic regression models. The STOMA score was developed and internally validated in a cohort of patients operated between 2014 and 2017, with subsequent temporal validation in a 2018 cohort. The discriminative power and calibration of the models' performance were evaluated.
Results: This study included 2499 patients with AL, 1954 in the development cohort and 545 in the validation cohort. Baseline characteristics were comparable. One-year stoma-free survival was 45.0% in the development cohort and 43.7% in the validation cohort. The following predictors were included in the STOMA score: sex, age, American Society of Anestesiologist classification, body mass index, clinical M-disease, neoadjuvant therapy, abdominal and transanal approach, primary defunctioning stoma, multivisceral resection, clinical setting in which AL was diagnosed, postoperative day of AL diagnosis, abdominal contamination, anastomotic defect circumference, bowel wall ischemia, anastomotic fistula, retraction, and reactivation leakage. The STOMA score showed good discrimination and calibration (c-index: 0.71, 95% CI: 0.66-0.76).
Conclusions: The STOMA score consists of 18 clinically relevant factors and estimates the individual risk for 1-year stoma-free survival in patients with AL after RC surgery, which may improve patient counseling and give guidance when analyzing the efficacy of different treatment strategies in future studies.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Borstlap WAA, Westerduin E, Aukema TS, et al. Anastomotic leakage and chronic presacral sinus formation after low anterior resection: results from a large cross-sectional study. Ann Surg. 2017;266:870–877. - PubMed
-
- Hughes DL, Cornish J, Morris C. Group LTM. Functional outcome following rectal surgery-predisposing factors for low anterior resection syndrome. Int J Colorectal Dis. 2017;32:691–697. - PubMed
-
- Foppa C, Ng SC, Montorsi M, et al. Anastomotic leak in colorectal cancer patients: new insights and perspectives. Eur J Surg Oncol. 2020;46:943–954. - PubMed
-
- Chiarello MM, Fransvea P, Cariati M, et al. Anastomotic leakage in colorectal cancer surgery. Surg Oncol. 2022;40:101708. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
