

Development and validation of a nomogram to predict the risk of renal replacement therapy among acute kidney injury patients in intensive care unit
- PMID: 37498349
- PMCID: PMC10581925
- DOI: 10.1007/s10157-023-02383-5
Development and validation of a nomogram to predict the risk of renal replacement therapy among acute kidney injury patients in intensive care unit
Abstract
Background: There are no universally accepted indications to initiate renal replacement therapy (RRT) among patients with acute kidney injury (AKI). This study aimed to develop a nomogram to predict the risk of RRT among AKI patients in intensive care unit (ICU).
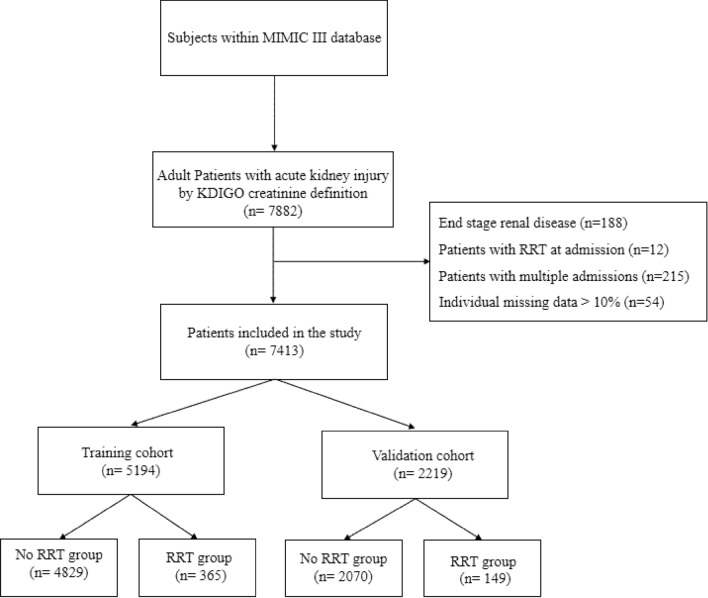
Methods: In this retrospective cohort study, we extracted AKI patients from Medical Information Mart for Intensive Care III (MIMIC-III) database. Patients were randomly divided into a training cohort (70%) and a validation cohort (30%). Multivariable logistic regression based on Akaike information criterion was used to establish the nomogram. The discrimination and calibration of the nomogram were evaluated by Harrell's concordance index (C-index) and Hosmer-Lemeshow (HL) test. Decision curve analysis (DCA) was performed to evaluate clinical application.
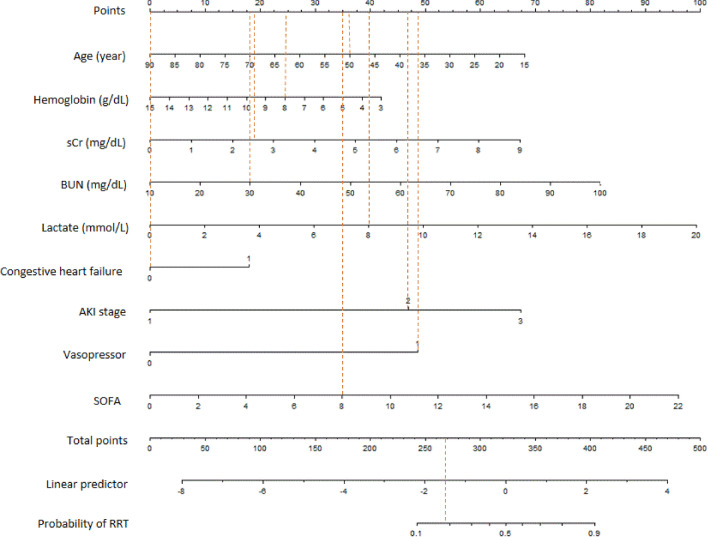
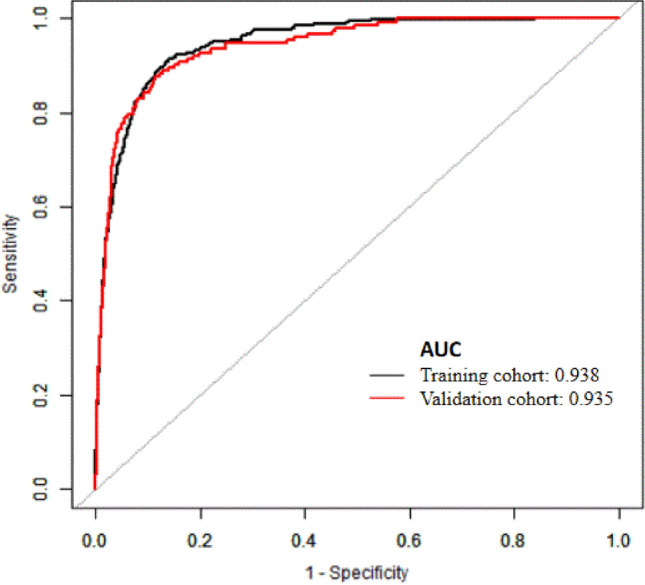
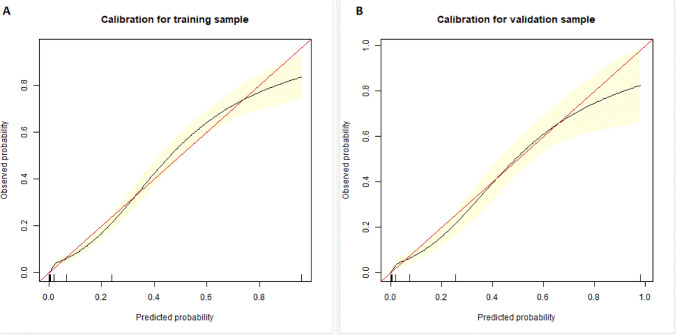
Results: A total of 7413 critically ill patients with AKI were finally enrolled. 514 (6.9%) patients received RRT after ICU admission. 5194 (70%) patients were in the training cohort and 2219 (30%) patients were in the validation cohort. Nine variables, namely, age, hemoglobin, creatinine, blood urea nitrogen and lactate at AKI detection, comorbidity of congestive heart failure, AKI stage, and vasopressor use were included in the nomogram. The predictive model demonstrated satisfying discrimination and calibration with C-index of 0.938 (95% CI, 0.927-0.949; HL test, P = 0.430) in training set and 0.935 (95% CI, 0.919-0.951; HL test, P = 0.392) in validation set. DCA showed a positive net benefit of our nomogram.
Conclusion: The nomogram developed in this study was highly accurate for RRT prediction with potential application value.
Keywords: Acute kidney injury; Intensive care unit; MIMIC-III database; Nomogram; Renal replacement therapy.
© 2023. The Author(s).
Conflict of interest statement
None of the authors has any potential conflicts of interest related to this article to declare, and the results of this report have been produced, analyzed, and interpreted without any outside participation.
Figures

References
-
- Zarbock A, Kellum JA, Schmidt C, Van Aken H, Wempe C, Pavenstädt H, et al. Effect of early vs delayed initiation of renal replacement therapy on mortality in critically ill patients with acute kidney injury: the ELAIN Randomized Clinical Trial. JAMA. 2016;315(20):2190–2199. doi: 10.1001/jama.2016.5828. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
