

Changing haemodynamic status of patients referred for transcatheter aortic valve intervention during the COVID-19 pandemic
- PMID: 37498468
- PMCID: PMC10516812
- DOI: 10.1007/s12471-023-01795-y
Changing haemodynamic status of patients referred for transcatheter aortic valve intervention during the COVID-19 pandemic
Erratum in
-
Publisher Correction to: Changing haemodynamic status of patients referred for transcatheter aortic valve intervention during the COVID-19 pandemic.Neth Heart J. 2023 Oct;31(10):412. doi: 10.1007/s12471-023-01808-w. Neth Heart J. 2023. PMID: 37665524 Free PMC article. No abstract available.
Abstract
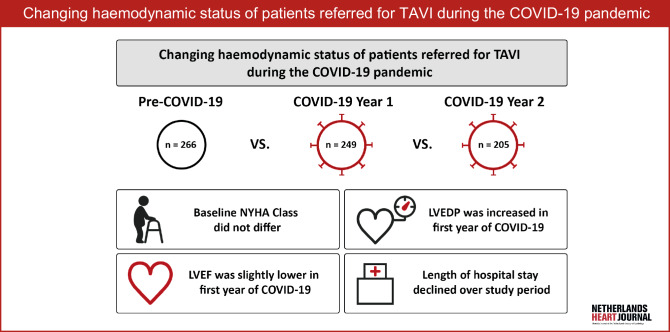
Introduction: Delays in the diagnosis and referral of aortic stenosis (AS) during the coronavirus disease 2019 (COVID-19) pandemic may have affected the haemodynamic status of AS patients. We aimed to compare clinical and haemodynamic characteristics of severe AS patients referred for transcatheter aortic valve implantation (TAVI) or balloon aortic valvuloplasty (BAV) before the pandemic versus two subsequent periods.
Methods: This study compared three 1‑year historical cohorts: a pre-COVID-19 group (PCOV), a 1st-year COVID-19 group (COV-Y1) and a 2nd-year COVID-19 group (COV-Y2). The main parameters were baseline New York Heart Association (NYHA) functional class, left ventricular ejection fraction (LVEF) and left ventricular end-diastolic pressure (LVEDP). Demographics, procedural characteristics and 30-day clinical outcomes were assessed. The transition time between heart team decision and TAVI was examined. Pairwise group comparisons were performed (PCOV vs COV-1Y and COV-1Y vs COV-2Y).
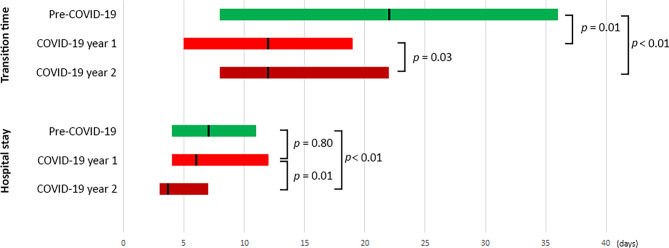
Results: A total of 720 patients were included with 266, 249 and 205 patients in the PCOV, COV-Y1 and COV-Y2 groups, respectively. BAV was performed in 28 patients (4%). NYHA class did not differ across the cohorts. Compared to PCOV, LVEF was slightly lower in COV-Y1 (58% (49-60%) vs 57% (45-60%), p = 0.03); no difference was observed when comparing COV-Y1 and COV-Y2. LVEDP was higher in COV-Y1 than in PCOV (20 mm Hg (16-26 mm Hg) vs 17 mm Hg (13-24 mm Hg), p = 0.01). No difference was found when comparing LVEDP between COV-Y1 and COV-Y2. Thirty-day mortality did not differ between groups. Transition time was reduced in the COVID era. Duration of hospital stay declined over the study period.
Conclusions: Patients undergoing TAVI during the COVID-19 pandemic had more advanced AS illustrated by lower LVEF and higher LVEDP, but there were no differences in clinical outcome. The TAVI pathway became more efficient.
Keywords: COVID-19; Haemodynamics; Transcatheter aortic valve implantation.
© 2023. The Author(s).
Conflict of interest statement
J. Daemen received institutional grant/research support from Astra Zeneca, Abbott Vascular, Boston Scientific, ACIST Medical, Medtronic, Pie Medical and ReCor Medical. N.M. Van Mieghem received research grant support from Abbott Vascular, Boston Scientific, Medtronic, Edwards Lifesciences, Daiichi Sankyo and PulseCath BV.J.F. Ooms, T.W. Hokken, R. Adrichem, D. Gunes, M. de Ronde-Tillmans, I. Kardys, J. Goudzwaard, F. Mattace-Raso and R.-J. Nuis declare that they have no competing interests.
Figures
Similar articles
-
Transcatheter Aortic Valve Implantation for Severe Bicuspid Aortic Stenosis - 2 Years Follow up Experience From India.Front Cardiovasc Med. 2022 Jul 28;9:817705. doi: 10.3389/fcvm.2022.817705. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35966565 Free PMC article.
-
Relation of preprocedural assessment of myocardial contractility reserve on outcomes of aortic stenosis patients with impaired left ventricular function undergoing transcatheter aortic valve implantation.Am J Cardiol. 2014 May 1;113(9):1536-42. doi: 10.1016/j.amjcard.2014.01.433. Epub 2014 Feb 13. Am J Cardiol. 2014. PMID: 24641965
-
Balloon aortic valvuloplasty for urgent treatment of severe aortic stenosis during coronavirus disease 2019 pandemic: a case report.ESC Heart Fail. 2020 Dec;7(6):4348-4352. doi: 10.1002/ehf2.13003. Epub 2020 Sep 19. ESC Heart Fail. 2020. PMID: 32949219 Free PMC article.
-
Sustained favourable haemodynamics 1 year after TAVI: improvement in NYHA functional class related to improvement of left ventricular diastolic function.Eur Heart J Cardiovasc Imaging. 2016 Nov;17(11):1269-1278. doi: 10.1093/ehjci/jev306. Epub 2015 Nov 20. Eur Heart J Cardiovasc Imaging. 2016. PMID: 26588980
-
Left ventricular end-diastolic pressure as an independent predictor of outcome during balloon aortic valvuloplasty.Catheter Cardiovasc Interv. 2014 Apr 1;83(5):782-8. doi: 10.1002/ccd.24410. Epub 2013 Dec 4. Catheter Cardiovasc Interv. 2014. PMID: 22511584 Free PMC article.
References
-
- Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72–e227. - PubMed
-
- Bruins B. First COVID-19 patient in the Netherlands [Government letter]. Dutch Ministry of Health, Welfare and Sport. 2020. https://open.overheid.nl/documenten/ronl-bc3dd8cc-396e-4746-b054-c016bf4.... Accessed January 27 2020
LinkOut - more resources
Full Text Sources
Research Materials
