

High sensitivity of asymmetric 18F-THK5351 PET abnormality in patients with corticobasal syndrome
- PMID: 37500734
- PMCID: PMC10374540
- DOI: 10.1038/s41598-023-39227-x
High sensitivity of asymmetric 18F-THK5351 PET abnormality in patients with corticobasal syndrome
Abstract
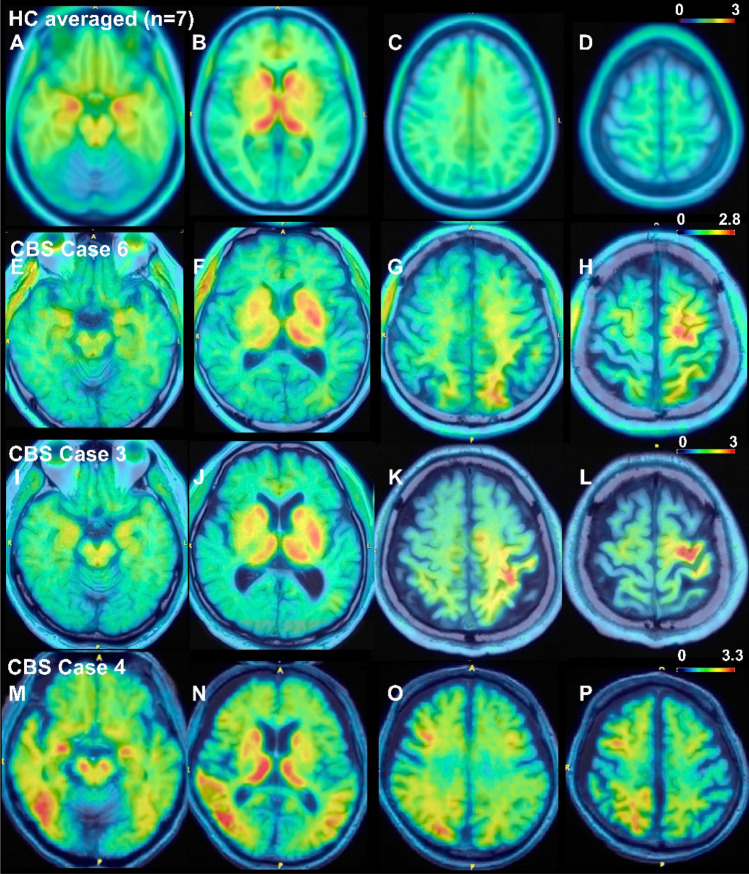
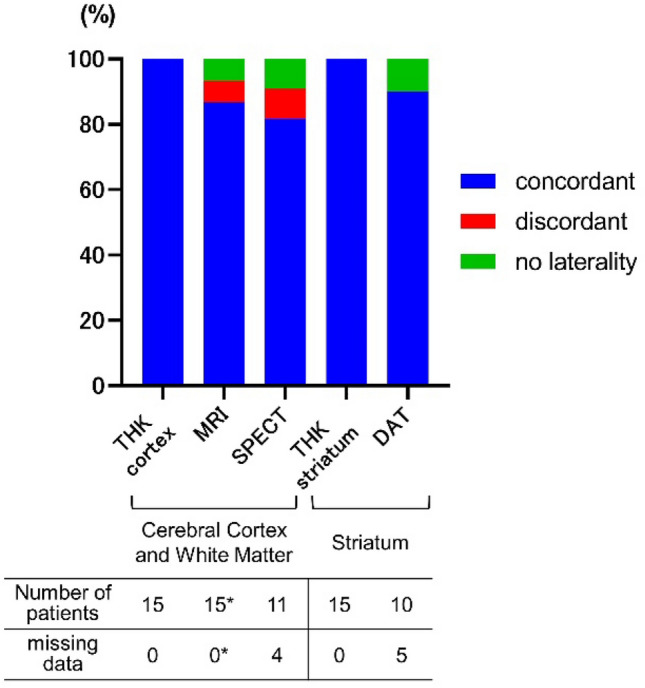
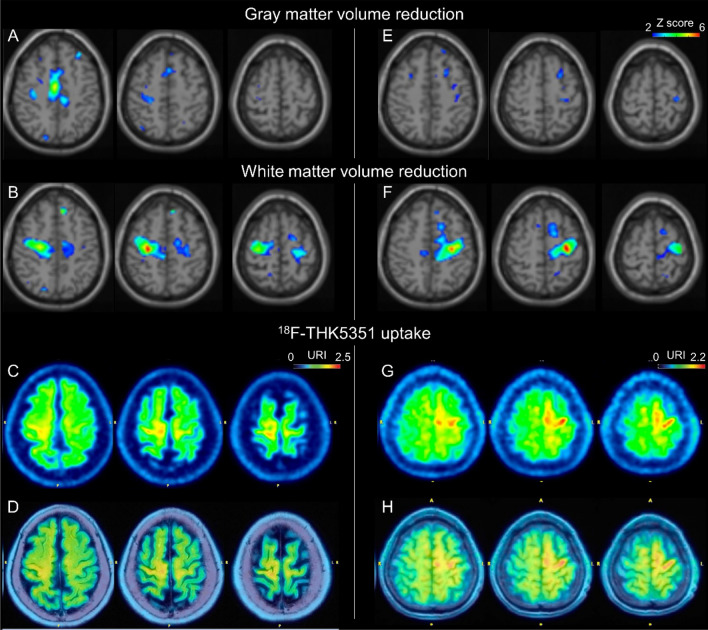
Corticobasal syndrome (CBS) is characterized by symptoms related to the asymmetric involvement of the cerebral cortex and basal ganglia. However, early detection of asymmetric imaging abnormalities can be challenging. Previous studies reported asymmetric 18F-THK5351 PET abnormalities in CBS patients, but the sensitivity for detecting such abnormalities in larger patient samples, including early-stage cases, remains unclear. Patients clinically diagnosed with CBS were recruited. All patients displayed asymmetric symptoms in the cerebral cortex and basal ganglia. Asymmetric THK5351 PET abnormalities were determined through visual assessment. Brain MRI, perfusion SPECT, and dopamine transporter (DAT) SPECT results were retrospectively reviewed. The 15 patients had a median age of 72 years (59-86 years) and a disease duration of 2 years (0.5-7 years). Four patients met the probable and 11 met the possible CBS criteria according to Armstrong criteria at the time of PET examination. All patients, including early-stage cases, exhibited asymmetric tracer uptake contralateral to their symptom-dominant side in the cerebral cortex/subcortical white matter and striatum (100%). The sensitivity for detecting asymmetric imaging abnormalities contralateral to the symptom-dominant side was 86.7% for brain MRI, 81.8% for perfusion SPECT, and 90% for DAT SPECT. White matter volume reduction was observed in the subcortical region of the precentral gyrus with increased THK5351 uptake, occurring significantly more frequently than gray matter volume reduction. THK5351 PET may be a sensitive imaging technique for detecting asymmetric CBS pathologies, including those in early stages.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
