

A reinforcement learning model for AI-based decision support in skin cancer
- PMID: 37501017
- PMCID: PMC10427421
- DOI: 10.1038/s41591-023-02475-5
A reinforcement learning model for AI-based decision support in skin cancer
Abstract
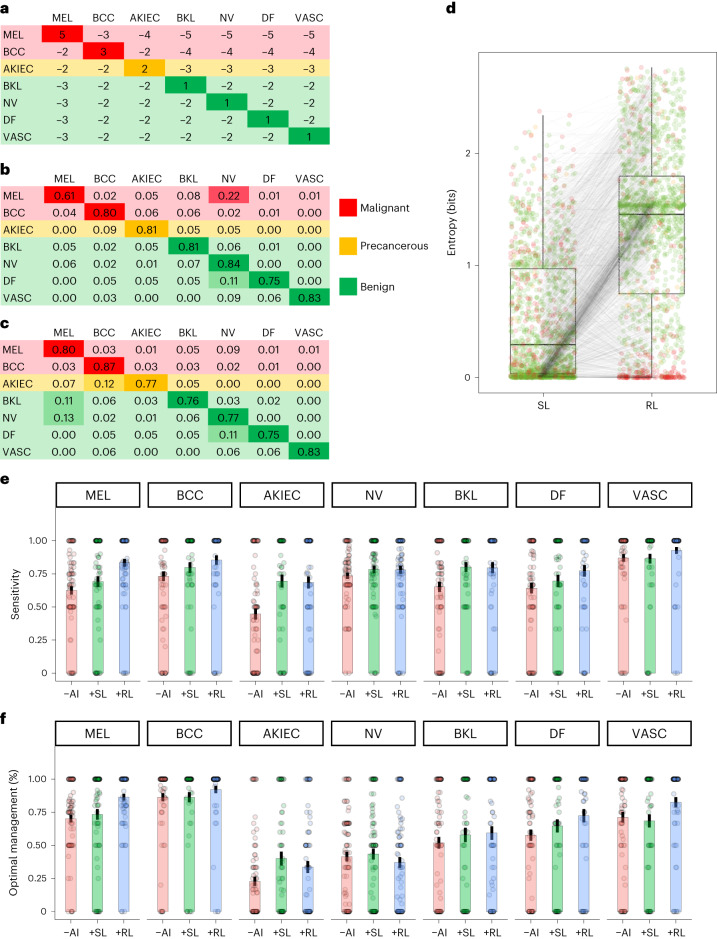
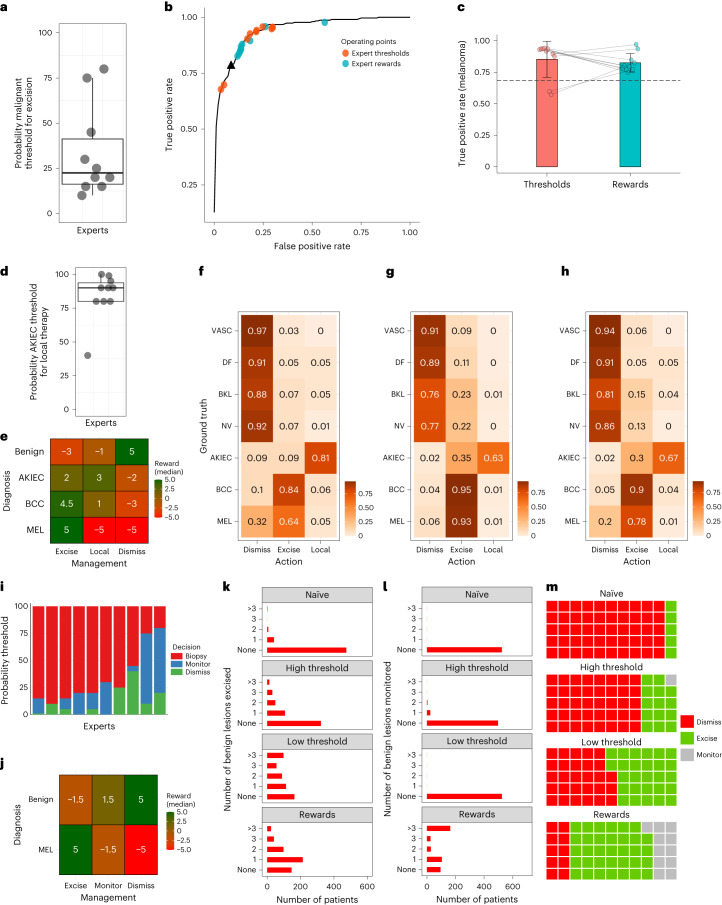
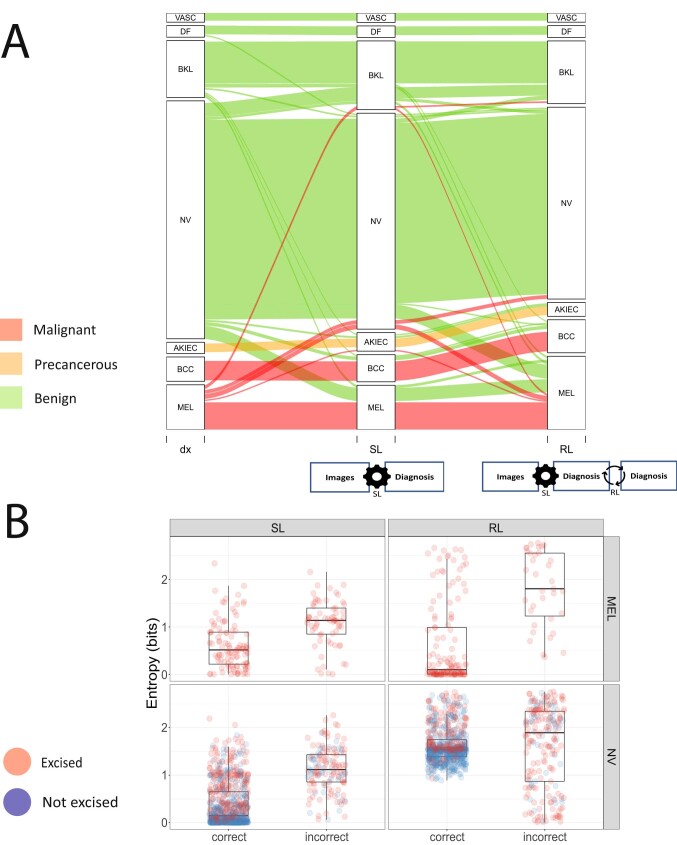
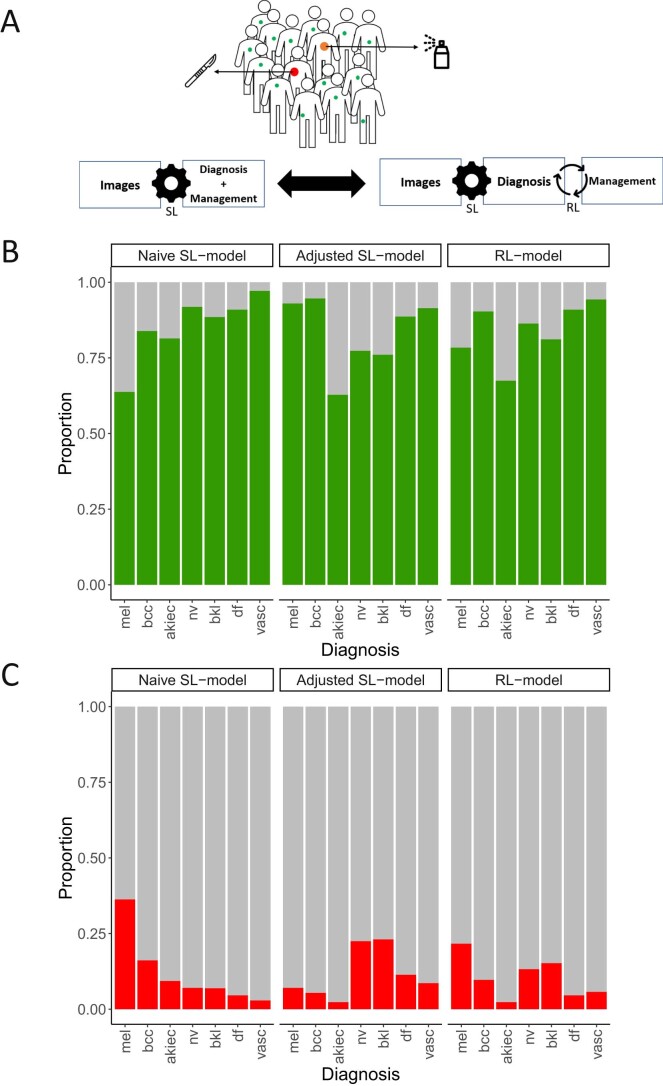
We investigated whether human preferences hold the potential to improve diagnostic artificial intelligence (AI)-based decision support using skin cancer diagnosis as a use case. We utilized nonuniform rewards and penalties based on expert-generated tables, balancing the benefits and harms of various diagnostic errors, which were applied using reinforcement learning. Compared with supervised learning, the reinforcement learning model improved the sensitivity for melanoma from 61.4% to 79.5% (95% confidence interval (CI): 73.5-85.6%) and for basal cell carcinoma from 79.4% to 87.1% (95% CI: 80.3-93.9%). AI overconfidence was also reduced while simultaneously maintaining accuracy. Reinforcement learning increased the rate of correct diagnoses made by dermatologists by 12.0% (95% CI: 8.8-15.1%) and improved the rate of optimal management decisions from 57.4% to 65.3% (95% CI: 61.7-68.9%). We further demonstrated that the reward-adjusted reinforcement learning model and a threshold-based model outperformed naïve supervised learning in various clinical scenarios. Our findings suggest the potential for incorporating human preferences into image-based diagnostic algorithms.
© 2023. The Author(s).
Conflict of interest statement
The authors declare the following competing interests: P.T. has received fees from Silverchair, speaker honoraria from FotoFinder, Lilly and Novartis, and an unrestricted one-year postdoc grant from MetaOptima Technology Inc. N.C. is a Microsoft employee and owns diverse investments across technology and healthcare companies. A.H. is a consultant to Canfield Scientific Inc. and advisory board member of Scibase AB. H.P.S. is a shareholder of MoleMap NZ Limited and e-derm consult GmbH and undertakes regular teledermatological reporting for both companies. H.P.S. is also a medical consultant for Canfield Scientific Inc., MoleMap Australia Pty Ltd, Blaze Bioscience Inc. and a medical adviser for First Derm. V.R. is a medical adviser for Inhabit Brands, Inc. H.K. received nonfinancial support from Derma Medical Systems, Fotofinder and Heine, and speaker fees from Fotofinder. The remaining authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
