

An updated meta-analysis of cardiac resynchronization therapy with or without defibrillation in patients with nonischemic cardiomyopathy
- PMID: 37502189
- PMCID: PMC10370697
- DOI: 10.3389/fcvm.2023.1078570
An updated meta-analysis of cardiac resynchronization therapy with or without defibrillation in patients with nonischemic cardiomyopathy
Abstract
Background: Cardiac resynchronization therapy (CRT) is a major device therapy used to treat patients suffering from heart failure (HF) and electrical asynchrony. It can improve HF symptoms, reduce HF hospitalization time, and improve long-term survival in HF with and without implantable cardioverter (ICD) therapy. However, the benefit of defibrillator therapy in CRT-eligible patients with nonischemic cardiomyopathy (NICM) remains unknown. As a result, we conducted a systematic review and meta-analysis to compare clinical outcomes in patients with NICM and HF who were treated with implantable CRT defibrillators (CRT-D) vs. a CRT pacemaker (CRT-P) alone.
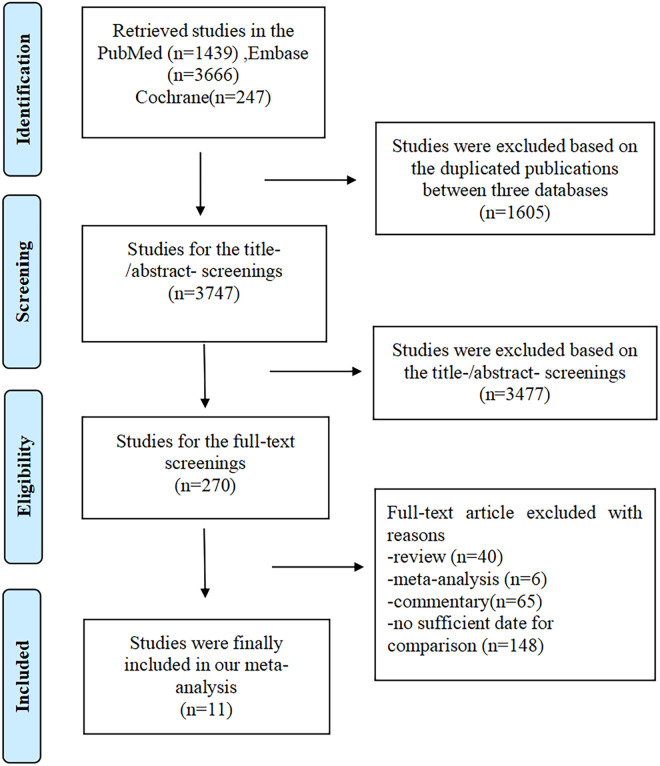
Methods: We searched the electronic databases PubMed, Embase, and Cochrane for all studies comparing CRT-D vs. CRT-P treatment in patients with NICM. The time frame was from 1990 to September 2022. All-cause mortality and cardiovascular mortality were the primary clinical outcomes of interest to us. To pool adjusted hazard ratios (HRs) and 95% confidence intervals (CIs), a random-effects model with inverse variance was used.
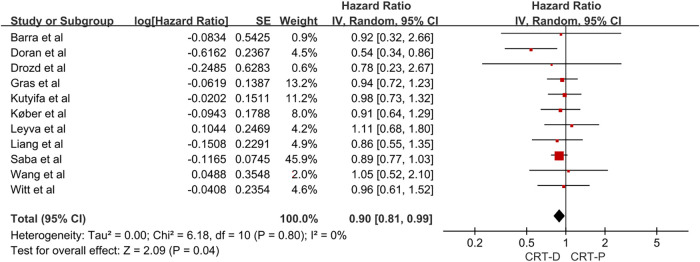
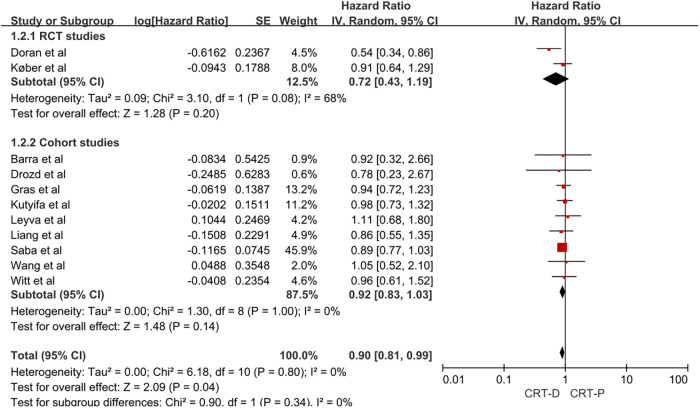
Results: A pooled meta-analysis included two randomized controlled trials (RCTs), each with 1,200 CRT-eligible patients with NICM (592 with CRT-D and 608 with CRT-P) and nine cohort studies representing 27,568 CRT-eligible patients with NICM (16,196 with CRT-D and 11,372 with CRT-P). The adjusted HR for all-cause mortality for CRT-D vs. CRT-P was 0.90 (95% CI, 0.81-0.99). In a subgroup analysis of two RCTs and nine cohort studies, the adjusted HR for all-cause mortality was 0.72 (95% CI, 0.43-1.19) and HR 0.92 (95% CI, 0.83-1.03) for CRT-D vs. CRT-P, respectively.
Conclusion: With the addition of defibrillation leads, we found a significantly lower risk of all-cause mortality in patients with NICM, but this association was not found in subgroup analyses of RCTs and observational studies.
Keywords: CRT defibrillators; CRT pacemaker; cardiac resynchronization therapy; heart failure; mortality; nonischemic cardiomyopathy.
© 2023 Liu, Gao and Luo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The Addition of a Defibrillator to Resynchronization Therapy Decreases Mortality in Patients With Nonischemic Cardiomyopathy.JACC Heart Fail. 2021 Jun;9(6):439-449. doi: 10.1016/j.jchf.2021.02.013. Epub 2021 May 12. JACC Heart Fail. 2021. PMID: 33992570 Clinical Trial.
-
Efficacy of Implantable Cardioverter-Defibrillator Therapy in Patients With Nonischemic Cardiomyopathy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.JACC Clin Electrophysiol. 2017 Sep;3(9):962-970. doi: 10.1016/j.jacep.2017.02.006. Epub 2017 May 31. JACC Clin Electrophysiol. 2017. PMID: 29759721
-
The benefits of defibrillator in heart failure patients with cardiac resynchronization therapy: A meta-analysis.Pacing Clin Electrophysiol. 2021 Feb;44(2):225-234. doi: 10.1111/pace.14150. Epub 2021 Jan 5. Pacing Clin Electrophysiol. 2021. PMID: 33372697
-
Implantable defibrillators for the prevention of mortality in patients with nonischemic cardiomyopathy: a meta-analysis of randomized controlled trials.JAMA. 2004 Dec 15;292(23):2874-9. doi: 10.1001/jama.292.23.2874. JAMA. 2004. PMID: 15598919 Review.
-
Implantable Cardioverter Defibrillators for Primary Prevention of Mortality in Patients With Nonischemic Cardiomyopathy: A Meta-Analysis of Randomized Controlled Trials.J Cardiovasc Electrophysiol. 2017 Jun;28(6):659-665. doi: 10.1111/jce.13204. Epub 2017 Apr 18. J Cardiovasc Electrophysiol. 2017. PMID: 28316104
Cited by
-
The impact of cardiac resynchronization therapy with implantable cardioverter defibrillators on patients with moderate to severe chronic heart failure: A single-arm clinical trial.Caspian J Intern Med. 2025 Mar 11;16(2):233-238. doi: 10.22088/cjim.16.2.233. eCollection 2025 Spring. Caspian J Intern Med. 2025. PMID: 40575746 Free PMC article.
-
Implantable Cardiac Devices in Patients with Brady- and Tachy-Arrhythmias: An Update of the Literature.Rev Cardiovasc Med. 2024 May 11;25(5):162. doi: 10.31083/j.rcm2505162. eCollection 2024 May. Rev Cardiovasc Med. 2024. PMID: 39076493 Free PMC article. Review.
References
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. Circulation. (2022) 145(18):e895–e1032. 10.1161/CIR.0000000000001062 - DOI - PubMed
-
- Linde C, Gold MR, Abraham WT, St JSM, Ghio S, Cerkvenik J, et al. Long-term impact of cardiac resynchronization therapy in mild heart failure: 5-year results from the REsynchronization reVErses remodeling in systolic left vEntricular dysfunction (REVERSE) study. Eur Heart J . (2013) 34(33):2592–9. 10.1093/eurheartj/eht160 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous