

A Case of an Early Pregnant Woman with Congenital Protein S Deficiency Who Underwent Mechanical Thrombectomy
- PMID: 37502450
- PMCID: PMC10370991
- DOI: 10.5797/jnet.cr.2020-0178
A Case of an Early Pregnant Woman with Congenital Protein S Deficiency Who Underwent Mechanical Thrombectomy
Abstract
Objective: Large vessel occlusion (LVO) stroke during pregnancy is rare but a life-threatening issue for the mother and fetus. We report a rare case of a pregnant woman with congenital protein S deficiency who underwent mechanical thrombectomy.
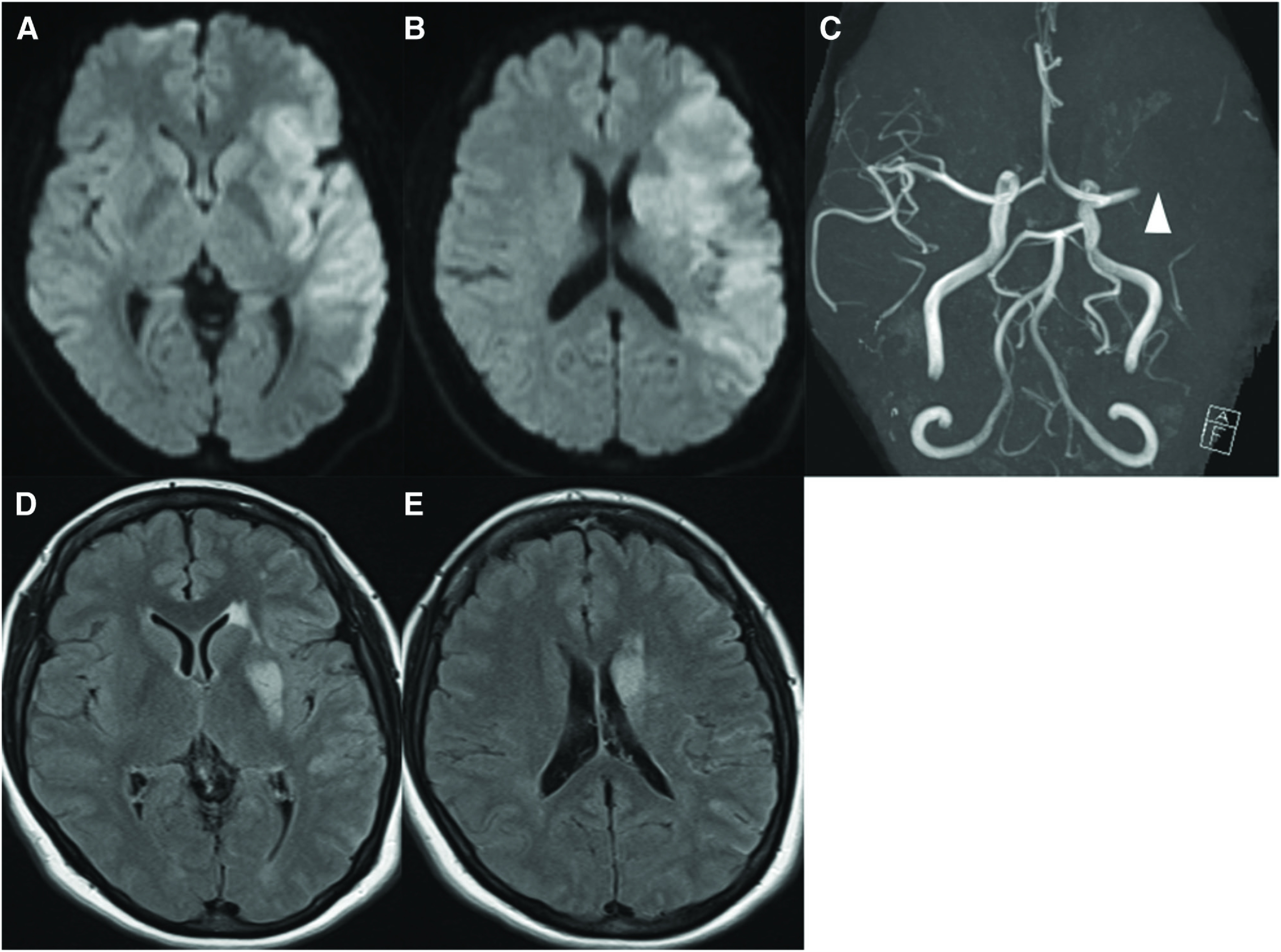
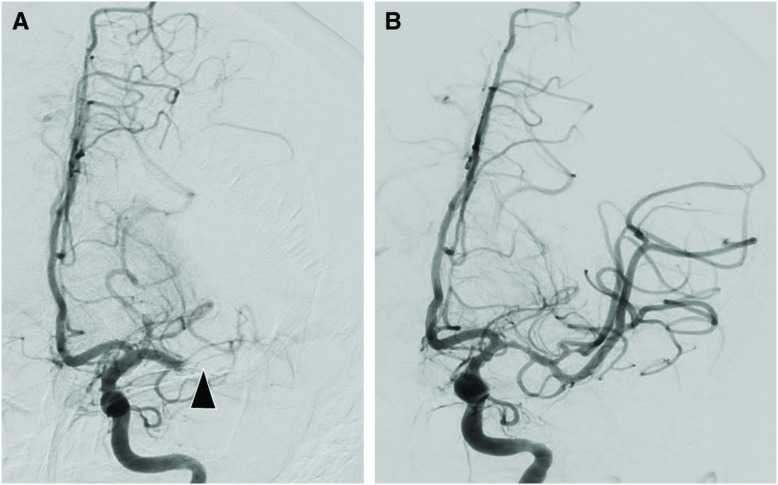
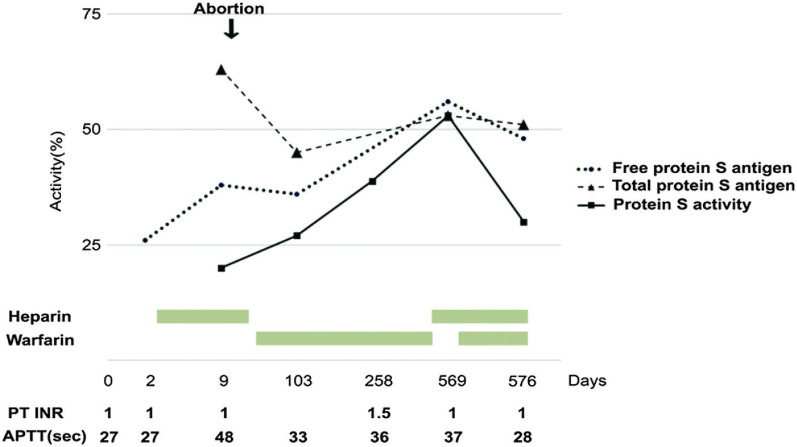
Case presentation: A 35-year-old woman presented with right hemiplegia and aphasia. The National Institutes of Health Stroke Scale was 23 and MRI revealed acute infarction on the left hemisphere. MRA showed disruption of the left middle cerebral artery. Mechanical thrombectomy was performed following intravenous thrombolysis, and then complete recanalization was achieved. The reduction in protein S activity due to pregnancy was suspected to have affected LVO. Subsequently, the patient was diagnosed with congenital protein S deficiency and recovered to modified Rankin scale 2 at 3 months after the onset.
Conclusion: Aggravation of congenital protein S deficiency due to pregnancy led to the onset of LVO. The patient showed a good outcome after mechanical thrombectomy.
Keywords: pregnancy; protein S; stroke; thrombectomy; tissue plasminogen activator.
©2022 The Japanese Society for Neuroendovascular Therapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Thrombolysis and Mechanical Thrombectomy for Acute Ischemic Stroke in Pregnancy: A Case Report.J Neuroendovasc Ther. 2021;15(2):124-128. doi: 10.5797/jnet.cr.2020-0102. Epub 2020 Sep 16. J Neuroendovasc Ther. 2021. PMID: 37502798 Free PMC article.
-
Mechanical thrombectomy for middle cerebral artery occlusion associated with ovarian hyperstimulation syndrome: case report and review of the literature.Ann Palliat Med. 2021 Mar;10(3):3504-3509. doi: 10.21037/apm-21-308. Epub 2021 Mar 17. Ann Palliat Med. 2021. PMID: 33752418 Review.
-
Mechanical Thrombectomy for Acute Medium Vessel Occlusion Because of Paradoxical Cerebral Embolism in a Patient with a Right Aortic Arch: A Case Report.J Neuroendovasc Ther. 2025;19(1):2024-0092. doi: 10.5797/jnet.cr.2024-0092. Epub 2025 Mar 29. J Neuroendovasc Ther. 2025. PMID: 40182579 Free PMC article.
-
Mechanical thrombectomy by Solitaire stent for treating acute ischemic stroke: A prospective cohort study.Int J Surg. 2016 Apr;28:2-7. doi: 10.1016/j.ijsu.2016.02.046. Epub 2016 Feb 15. Int J Surg. 2016. PMID: 26892715
-
Uneventful Pregnancy and Delivery after Thrombolysis Plus Thrombectomy for Acute Ischemic Stroke: Case Study and Literature Review.J Stroke Cerebrovasc Dis. 2019 Jan;28(1):70-75. doi: 10.1016/j.jstrokecerebrovasdis.2018.09.002. Epub 2018 Sep 27. J Stroke Cerebrovasc Dis. 2019. PMID: 30268366 Review.
References
-
- Swartz RH, Cayley ML, Foley N, et al. . The incidence of pregnancy-related stroke: a systematic review and meta-analysis. Int J Stroke 2017; 12: 687–697. - PubMed
-
- Kuklina EV, Tong X, Bansil P, et al. . Trends in pregnancy hospitalizations that included a stroke in the United States from 1994 to 2007: reasons for concern? Stroke 2011; 42: 2564–2570. - PubMed
-
- Yoshida K, Takahashi JC, Takenobu Y. Strokes associated with pregnancy and puerperium: a nationwide study by the Japan Stroke Society. Stroke 2017; 48: 276–282. - PubMed
-
- ten Kate MK, van der Meer J. Protein S deficiency: a clinical perspective. Haemophilia 2008; 14: 1222–1228. - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. . 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2018; 49: e46–e110. - PubMed