

Transarterial and Transvenous Coil Embolization of Direct Carotid-Cavernous Fistulas
- PMID: 37502641
- PMCID: PMC10370968
- DOI: 10.5797/jnet.tn.2020-0115
Transarterial and Transvenous Coil Embolization of Direct Carotid-Cavernous Fistulas
Abstract
Objective: Transvenous embolization (TVE) is typically used in combination with the residual shunt of transarterial embolization (TAE) for the treatment of direct carotid-cavernous fistulas (direct CCFs). This report is about our additional embolization method using combination therapy.
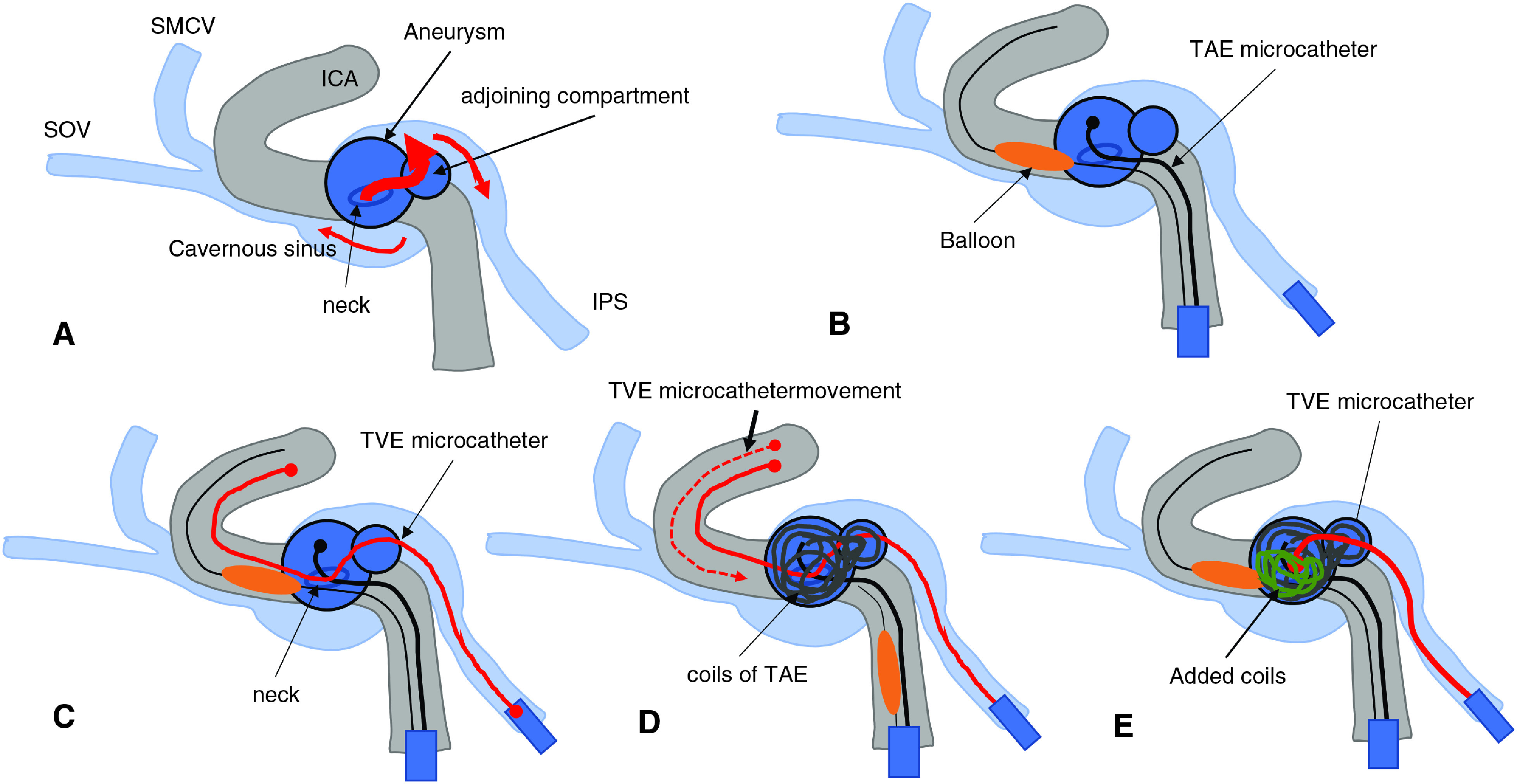
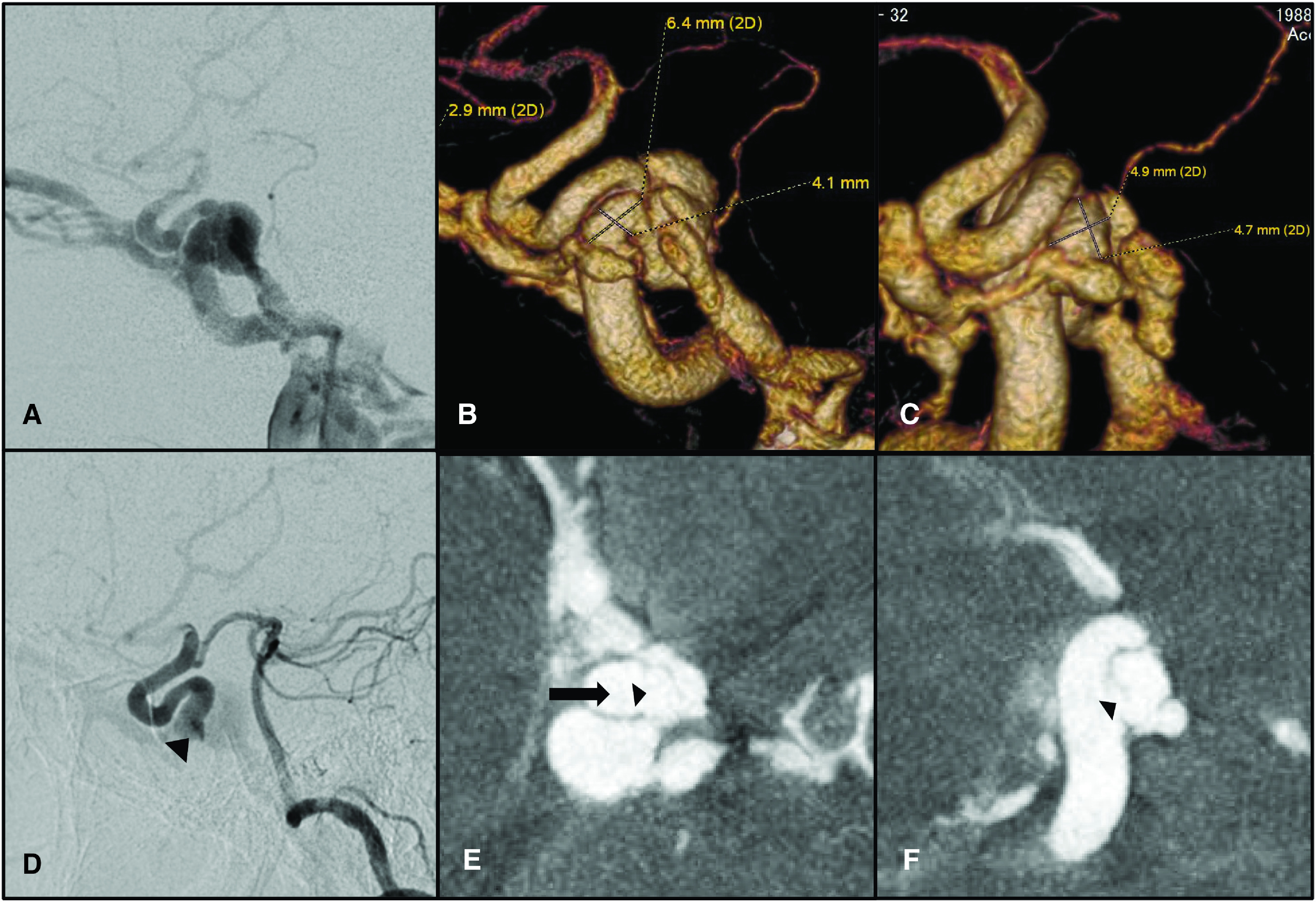
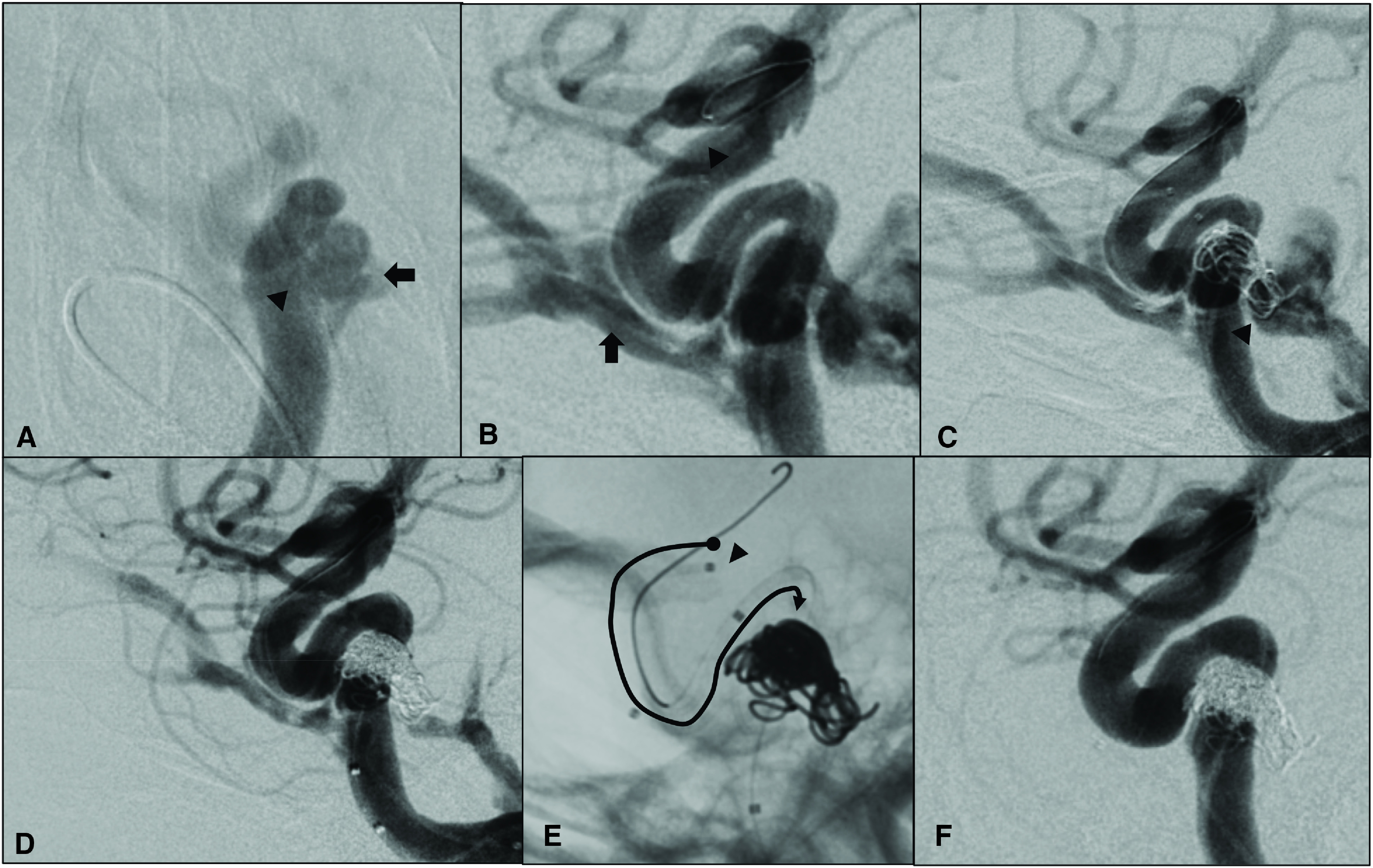
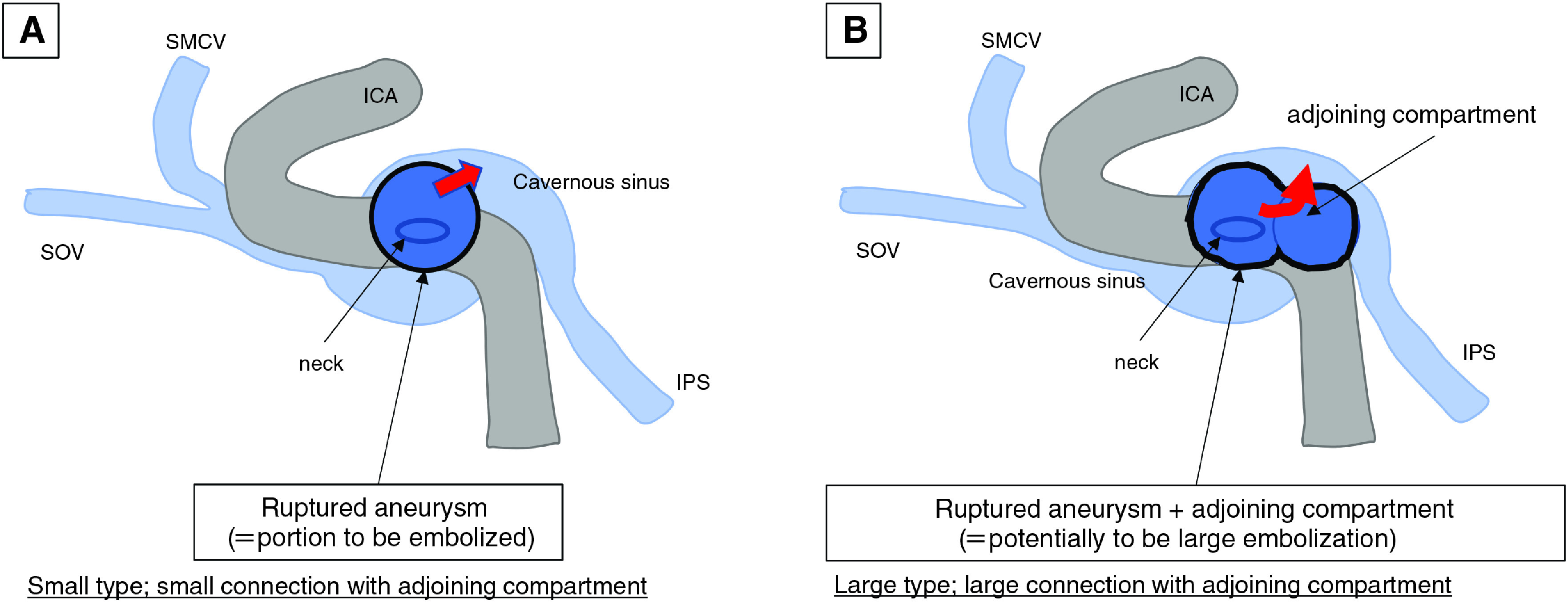
Case presentation: Five consecutive cases of direct CCF were presented; two were caused by aneurysms and three by head injuries. The treatment for each was started with TAE, with the addition of TVE if a shunt remained. At the time of TVE, a microcatheter positioned in the internal carotid artery passing from the cavernous sinus through the aneurysm neck or fistula was pulled back (pull-back method). It was then placed in the coil mass with TAE, and additional coils were filled. In two cases, the shunt disappeared by using only TAE, whereas it disappeared after being additionally embolized by the pull-back method in the remaining cases. All patients recovered with no postoperative complications.
Conclusion: The TAE and TVE combination therapy with the pull-back method could efficiently embolize the residual shunt after TAE.
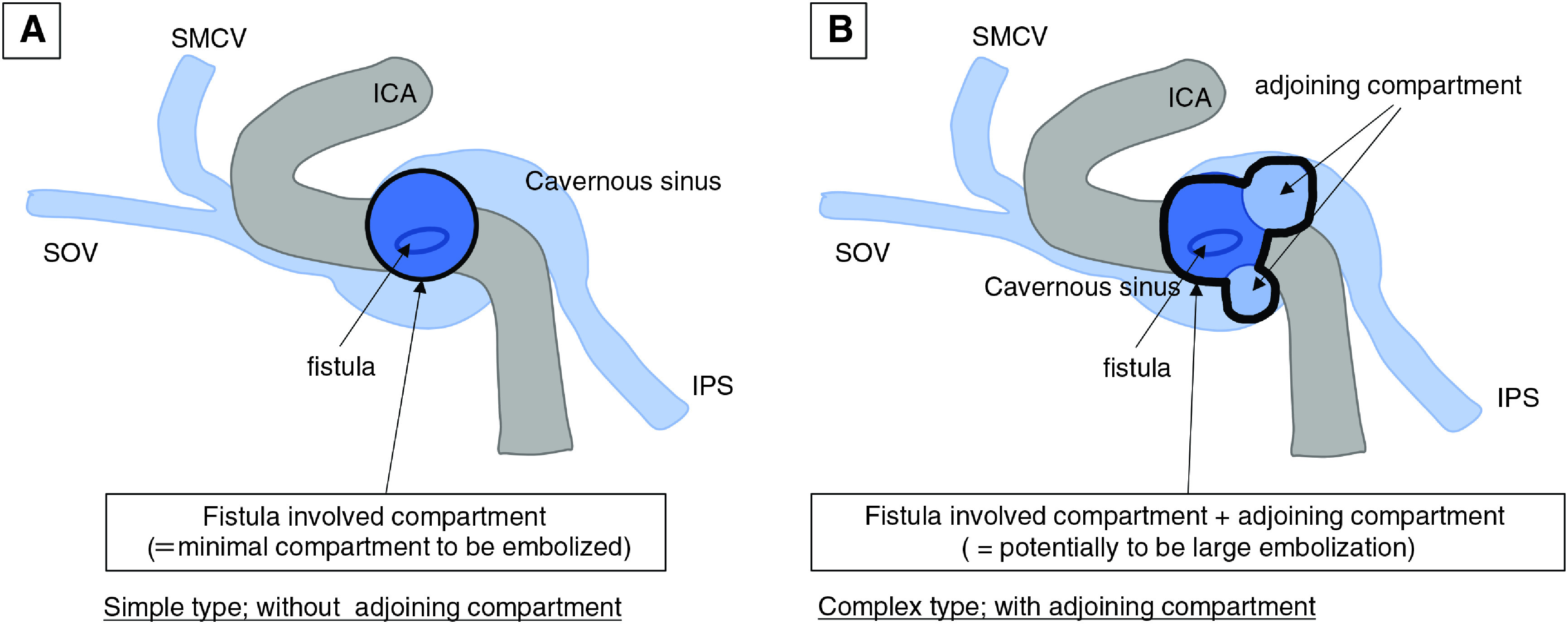
Keywords: cavernous sinus packing; detachable coils; fistula involved compartment; transfistula catheterization.
©2022 The Japanese Society for Neuroendovascular Therapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Direct carotid-cavernous fistula completely treated with a small number of coils by combined transarterial and transvenous embolization: A case report.Surg Neurol Int. 2025 Jan 17;16:14. doi: 10.25259/SNI_950_2024. eCollection 2025. Surg Neurol Int. 2025. PMID: 39926452 Free PMC article.
-
Transvenous embolization with a combination of detachable coils and Onyx for a complicated cavernous dural arteriovenous fistula.Chin Med J (Engl). 2008 Sep 5;121(17):1651-5. Chin Med J (Engl). 2008. PMID: 19024093
-
The evolution of endovascular treatment of carotid cavernous fistulas: a single-center experience.World Neurosurg. 2013 Nov;80(5):538-48. doi: 10.1016/j.wneu.2013.02.033. Epub 2013 Feb 9. World Neurosurg. 2013. PMID: 23402868
-
Direct Carotid Cavernous Fistulas.J Neuroendovasc Ther. 2020;14(12):583-592. doi: 10.5797/jnet.ra.2020-0131. Epub 2020 Nov 25. J Neuroendovasc Ther. 2020. PMID: 37502141 Free PMC article. Review.
-
Carotid cavernous fistula (CCF) treatment approaches: A systematic literature review and meta-analysis of transarterial and transvenous embolization for direct and indirect CCFs.Clin Neurol Neurosurg. 2021 May;204:106601. doi: 10.1016/j.clineuro.2021.106601. Epub 2021 Mar 20. Clin Neurol Neurosurg. 2021. PMID: 33774507
Cited by
-
Direct carotid-cavernous fistula completely treated with a small number of coils by combined transarterial and transvenous embolization: A case report.Surg Neurol Int. 2025 Jan 17;16:14. doi: 10.25259/SNI_950_2024. eCollection 2025. Surg Neurol Int. 2025. PMID: 39926452 Free PMC article.
-
Delayed Pontomesencephalic and Cervical Cord Venous Drainage Followed by Contralateral Carotid-Cavernous Fistula after Craniofacial Fractures: A Case Report.Neurointervention. 2024 Nov;19(3):185-189. doi: 10.5469/neuroint.2024.00318. Epub 2024 Oct 14. Neurointervention. 2024. PMID: 39390950 Free PMC article.
-
Transcirculation repair of a direct carotid-cavernous fistula in a patient who presented with hydrocephalus: illustrative case.J Neurosurg Case Lessons. 2025 Jan 27;9(4):CASE24618. doi: 10.3171/CASE24618. Print 2025 Jan 27. J Neurosurg Case Lessons. 2025. PMID: 39869896 Free PMC article.
References
-
- Ito Y, Satow T, Matsubara H, et al. . Selective shunt occlusion of direct carotid-cavernous fistula with vascular Ehlers-Danlos syndrome by multidevice technique: a case report and technical note. World Neurosurg 2019; 122: 123–128. - PubMed
-
- Kojima A, Onozuka S, Ishikawa M, et al. . Usefulness of the ED coil inifini for the treatment of direct carotid-cavernous fistula: technical note. JNET J Neuroendovasc Ther 2012; 6: 61–67.