

Arterial Spin Labeling Was Useful for Evaluating the Treatment Response of a Transverse-Sigmoid Sinus Dural Arteriovenous Fistula: A Case Report
- PMID: 37502803
- PMCID: PMC10370806
- DOI: 10.5797/jnet.cr.2019-0119
Arterial Spin Labeling Was Useful for Evaluating the Treatment Response of a Transverse-Sigmoid Sinus Dural Arteriovenous Fistula: A Case Report
Abstract
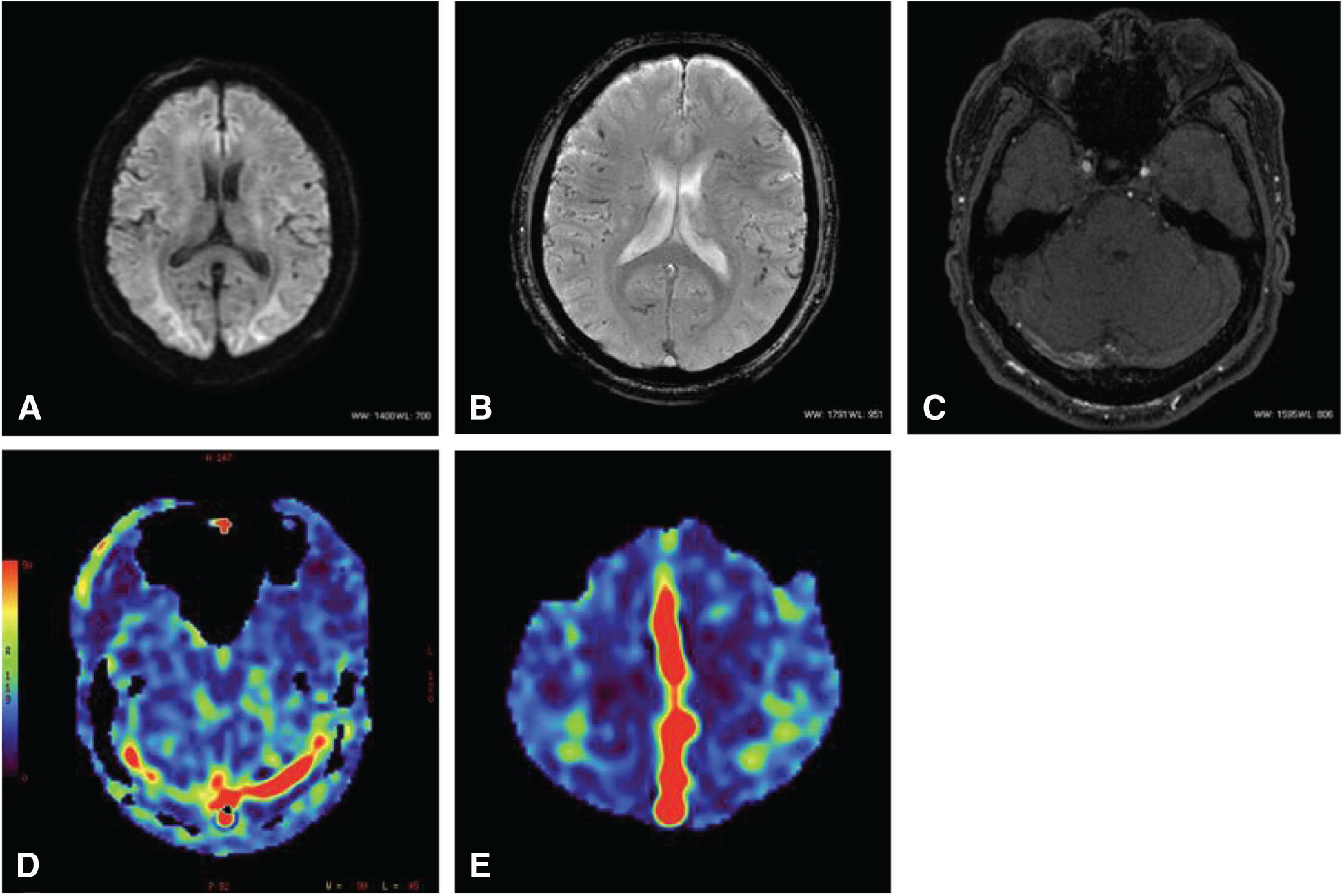
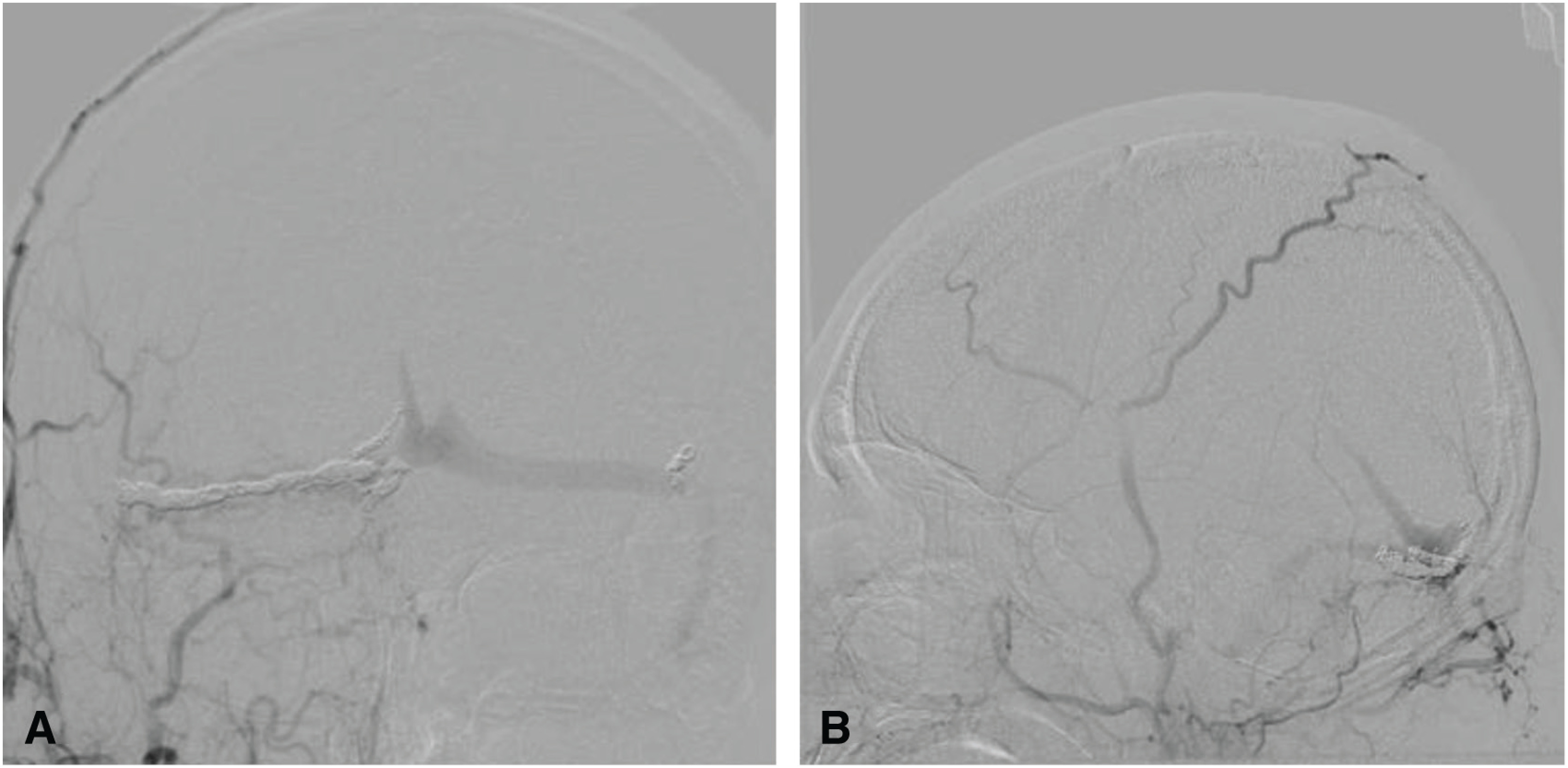
Objective: We report the case of a patient in whom arterial spin labeling (ASL) was useful for assessing the effects of treatment for a transverse-sigmoid sinus dural arteriovenous fistula (TSS-dAVF).
Case presentation: The patient was a 65-year-old man. Cerebral angiography demonstrated an aggressive dAVF involving the TSS, superior sagittal sinus (SSS), and the sinus confluence, with severe cortical and deep venous reflux. We performed multiple transarterial and transvenous embolizations for the TSS and sinus confluence lesion. The shunt disappeared almost completely after embolization. A high signal intensity that had been apparent in the SSS and straight sinus (StS) on ASL imaging before embolization disappeared after embolization. ASL imaging 3 months after embolization revealed slightly a high signal intensity in the StS, which was considered to be due to recurrence of the lesion. Moreover, recurrence of the confluence and TSS-dAVF was observed on cerebral angiography 6 months after embolization. As additional embolization was considered difficult, radiation therapy was recommended, but the patient refused; therefore, follow-up was performed. As ASL imaging findings were consistent with cerebral angiography findings, careful examination and monitoring of changes on ASL imaging were subsequently performed.
Conclusion: Follow-up using ASL imaging is useful to assess the effects of treatment performed for a dAVF.
Keywords: arterial spin labeling; dural arteriovenous fistula.
©2021 The Japanese Society for Neuroendovascular Therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
Fatal Hemorrhage Immediately after Transvenous Embolization of Transverse-sigmoid Sinus Dural Arteriovenous Fistulas: A Case Report.J Neuroendovasc Ther. 2020;14(8):319-325. doi: 10.5797/jnet.cr.2019-0101. Epub 2020 Jun 5. J Neuroendovasc Ther. 2020. PMID: 37502171 Free PMC article.
-
Single-session hematoma removal and transcortical venous approach for coil embolization of an isolated transverse-sigmoid sinus dural arteriovenous fistula in a hybrid operating room: illustrative case.J Neurosurg Case Lessons. 2022 May 23;3(21):CASE2267. doi: 10.3171/CASE2267. eCollection 2022 May 23. J Neurosurg Case Lessons. 2022. PMID: 35734231 Free PMC article.
-
An Onyx tunnel: reconstructive transvenous balloon-assisted Onyx embolization for dural arteriovenous fistula of the transverse-sigmoid sinus.J Neurosurg. 2018 Oct;129(4):922-927. doi: 10.3171/2017.5.JNS17287. Epub 2017 Nov 17. J Neurosurg. 2018. PMID: 29148903
-
Hypofractionated stereotactic radiosurgery for dural arteriovenous fistula in the superior sagittal sinus: case report and review of the literature.Br J Neurosurg. 2023 Aug;37(4):781-785. doi: 10.1080/02688697.2019.1648753. Epub 2019 Aug 9. Br J Neurosurg. 2023. PMID: 31397171 Review.
-
Transverse-sigmoid sinus dural arteriovenous fistula presenting with parkinsonism.Neurol Med Chir (Tokyo). 2013;53(4):224-7. doi: 10.2176/nmc.53.224. Neurol Med Chir (Tokyo). 2013. PMID: 23615412 Review.
Cited by
-
Evaluating post-treatment residual intracranial arteriovenous shunting: a comparison of arterial spin labeling MRI and digital subtraction angiography.Neuroradiology. 2025 May;67(5):1233-1250. doi: 10.1007/s00234-025-03548-7. Epub 2025 Feb 6. Neuroradiology. 2025. PMID: 39912896 Free PMC article.
References
-
- Chalela JA, Alsop DC, Gonzalez-Atavales JB, et al. : Magnetic resonance perfusion imaging in acute ischemic stroke using continuous arterial spin labeling. Stroke 2000; 31: 680–687. - PubMed
-
- Amukotuwa SA, Heit JJ, Marks MP, et al. : Detection of cortical venous drainage and determination of the borden type of dural arteriovenous fistula by means of 3D pseudocontinuous arterial spin-labeling MRI. AJR AM J Roentgenol 2016; 207: 163–169. - PubMed
-
- Kuwayama N: Epidemiologic survey of dural arteriovenous fistulas in Japan: clinical frequency and present status of treatment. Acta Neurochir Suppl 2016; 123: 185–188. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials