

This is a preprint.
Inflammation induced by tumor-associated nerves promotes resistance to anti-PD-1 therapy in cancer patients and is targetable by interleukin-6 blockade
- PMID: 37503252
- PMCID: PMC10371163
- DOI: 10.21203/rs.3.rs-3161761/v1
Inflammation induced by tumor-associated nerves promotes resistance to anti-PD-1 therapy in cancer patients and is targetable by interleukin-6 blockade
Update in
-
Cancer-induced nerve injury promotes resistance to anti-PD-1 therapy.Nature. 2025 Oct;646(8084):462-473. doi: 10.1038/s41586-025-09370-8. Epub 2025 Aug 20. Nature. 2025. PMID: 40836096 Free PMC article.
Abstract
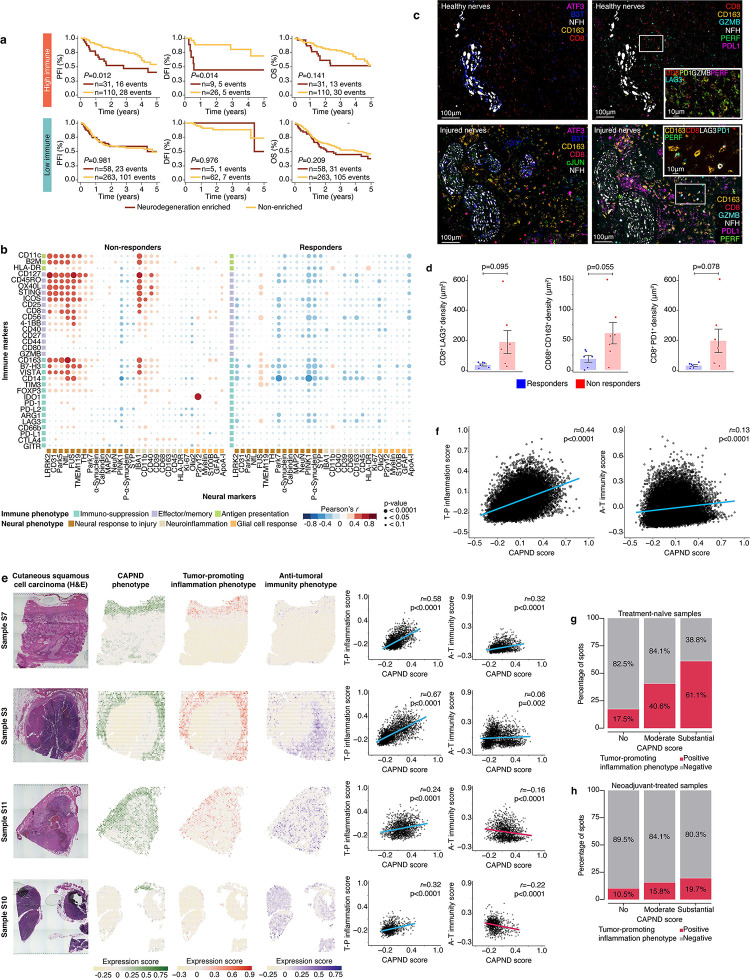
While the nervous system has reciprocal interactions with both cancer and the immune system, little is known about the potential role of tumor associated nerves (TANs) in modulating anti-tumoral immunity. Moreover, while peri-neural invasion is a well establish poor prognostic factor across cancer types, the mechanisms driving this clinical effect remain unknown. Here, we provide clinical and mechniastic association between TANs damage and resistance to anti-PD-1 therapy. Using electron microscopy, electrical conduction studies, and tumor samples of cutaneous squamous cell carcinoma (cSCC) patients, we showed that cancer cells can destroy myelin sheath and induce TANs degeneration. Multi-omics and spatial analyses of tumor samples from cSCC patients who underwent neoadjuvant anti-PD-1 therapy demonstrated that anti-PD-1 non-responders had higher rates of peri-neural invasion, TANs damage and degeneration compared to responders, both at baseline and following neoadjuvant treatment. Tumors from non-responders were also characterized by a sustained signaling of interferon type I (IFN-I) - known to both propagate nerve degeneration and to dampen anti-tumoral immunity. Peri-neural niches of non-responders were characterized by higher immune activity compared to responders, including immune-suppressive activity of M2 macrophages, and T regulatory cells. This tumor promoting inflammation expanded to the rest of the tumor microenvironment in non-responders. Anti-PD-1 efficacy was dampened by inducing nerve damage prior to treatment administration in a murine model. In contrast, anti-PD-1 efficacy was enhanced by denervation and by interleukin-6 blockade. These findings suggested a potential novel anti-PD-1 resistance drived by TANs damage and inflammation. This resistance mechanism is targetable and may have therapeutic implications in other neurotropic cancers with poor response to anti-PD-1 therapy such as pancreatic, prostate, and breast cancers.
Conflict of interest statement
Conflict of interests Kenneth Tsai serves as a consultant to NFlection Therapeutics, Sun Pharma, DXB Biosciences. Renata Ferrarotto reports Consulting or Advisory Role: Regeneron, Sanofi, Elevar Therapeutics, Remix, Eisai, Bioatlas, Coherus in the past 24 months and research Funds (Inst): Prelude, Ayala, Merck, Pfizer, Rakuten, EMD Serono, ISA, Viracta, and Gilead in the past 24 months. Neil Gross reports consulting for Intuitive Surgical, Sanofi-Genzyme, Regeneron, DragonFly Therapeutics, Merck and PDS Biotechnology. Michael A Davies has been a consultant to Roche/Genentech, Array, Pfizer, Novartis, BMS, GSK, Sanofi-Aventis, Vaccinex, Apexigen, Eisai, Iovance, Merck, and ABM Therapeutics, and he has been the PI of research grants to MD Anderson by Roche/Genentech, GSK, Sanofi-Aventis, Merck, Myriad, Oncothyreon, Pfizer, ABM Therapeutics, and LEAD Pharma. Jennifer Wargo is an inventor on a US patent application (PCT/US17/53.717) submitted by the University of Texas MD Anderson Cancer Center which covers methods to enhance immune checkpoint blockade responses by modulating the microbiome, reports compensation for speaker’s bureau and honoraria from Imedex, Dava Oncology, Omniprex, Illumina, Gilead, PeerView, Physician Education Resource, MedImmune, Exelixis and Bristol Myers Squibb, and has served as a consultant/advisory board member for Roche/Genentech, Novartis, AstraZeneca, GlaxoSmithKline, Bristol Myers Squibb, Micronoma, OSE therapeutics, Merck, and Everimmune. Dr. Wargo receives stock options from Micronoma and OSE therapeutics.
Figures



References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
