

This is a preprint.
Novel CSF tau biomarkers can be used for disease staging of sporadic Alzheimer's disease
- PMID: 37503281
- PMCID: PMC10370223
- DOI: 10.1101/2023.07.14.23292650
Novel CSF tau biomarkers can be used for disease staging of sporadic Alzheimer's disease
Abstract
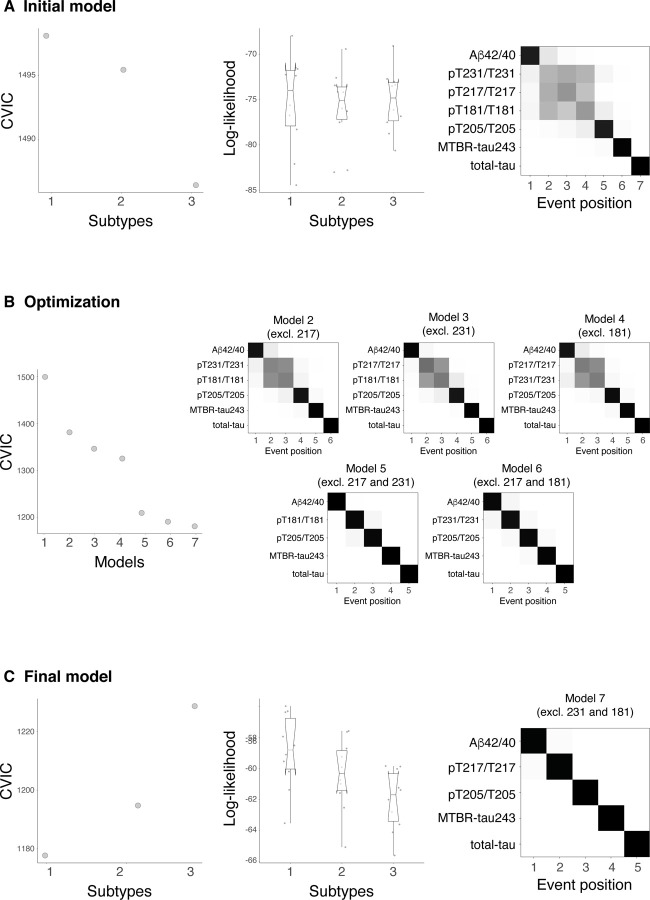
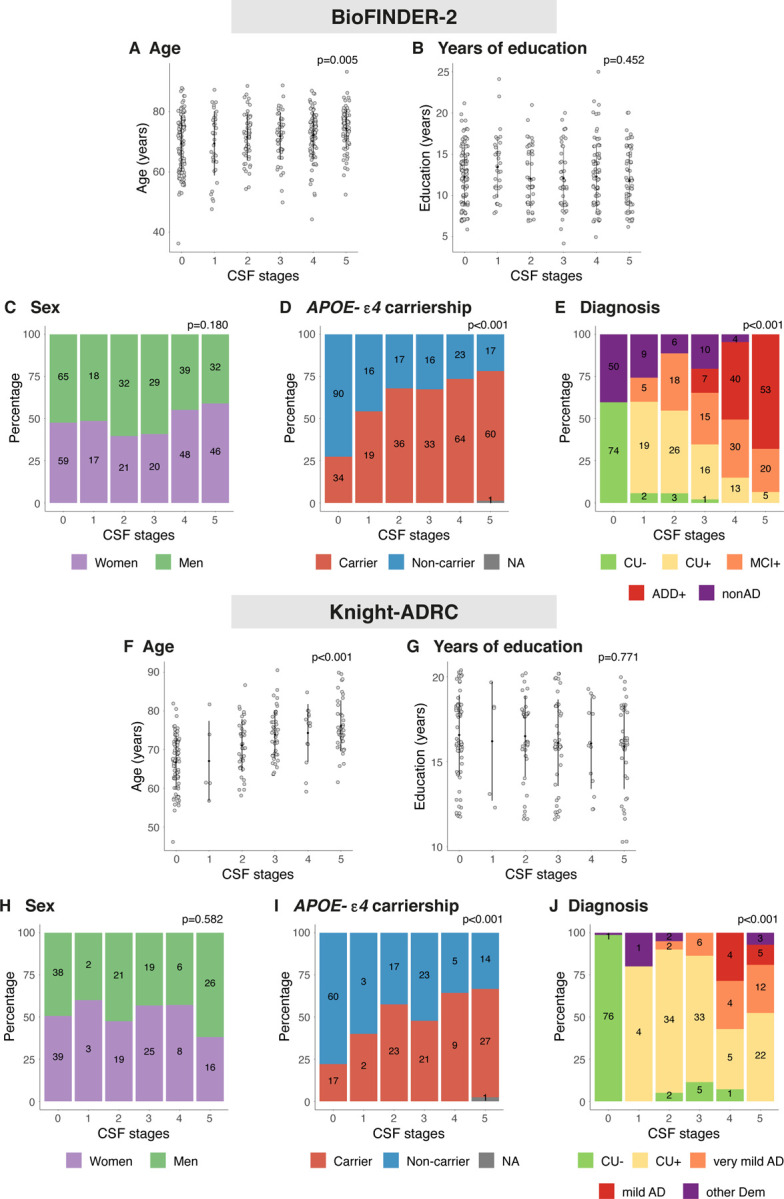
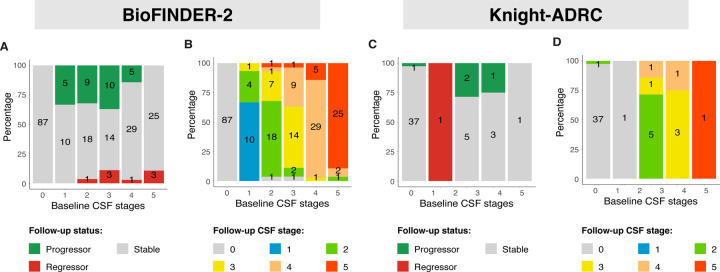
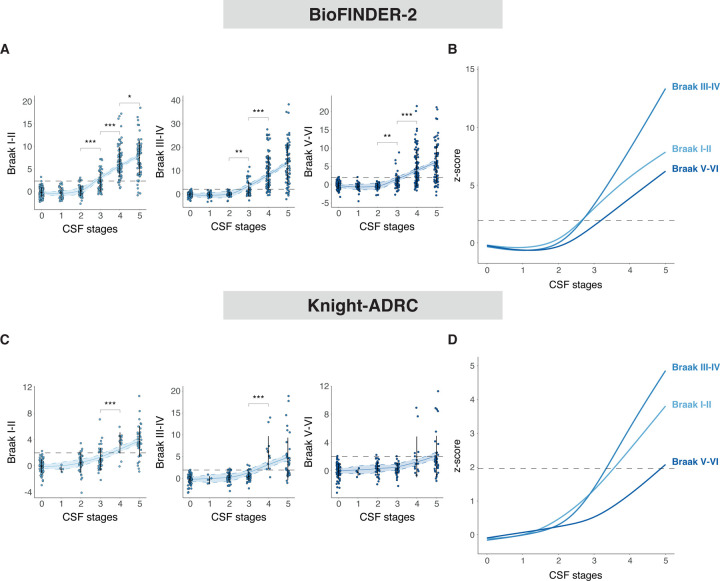
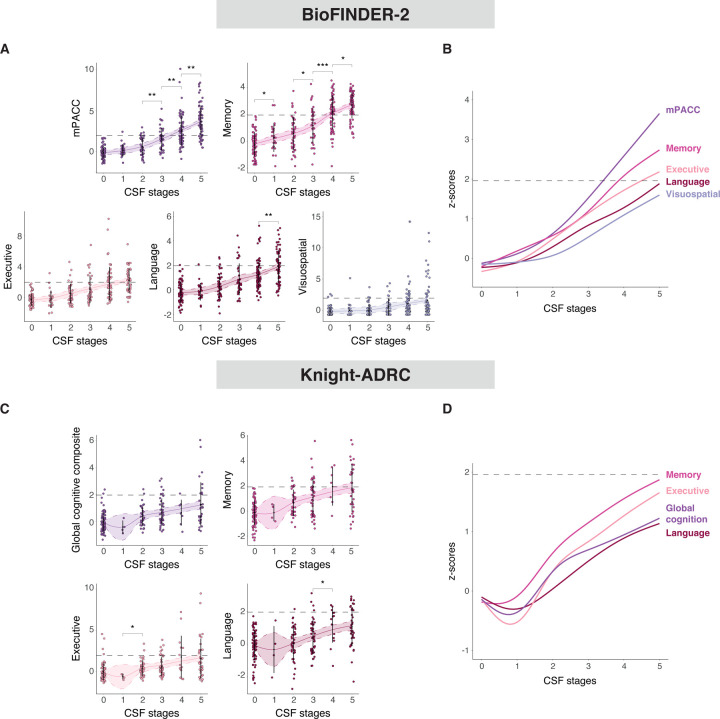
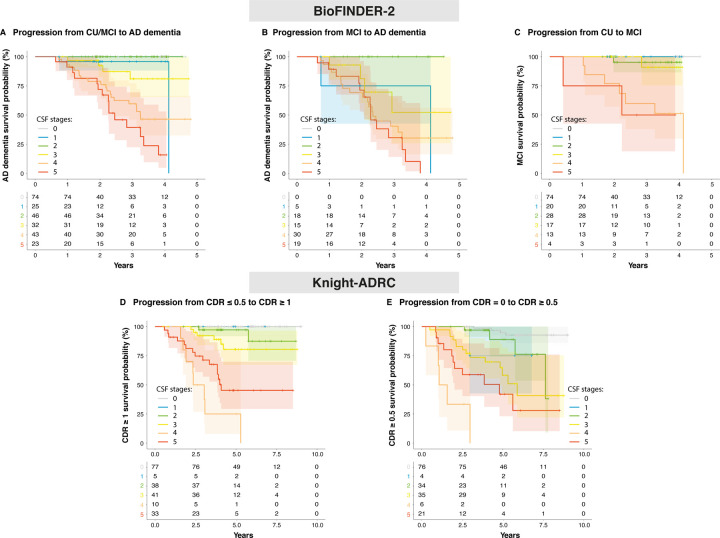
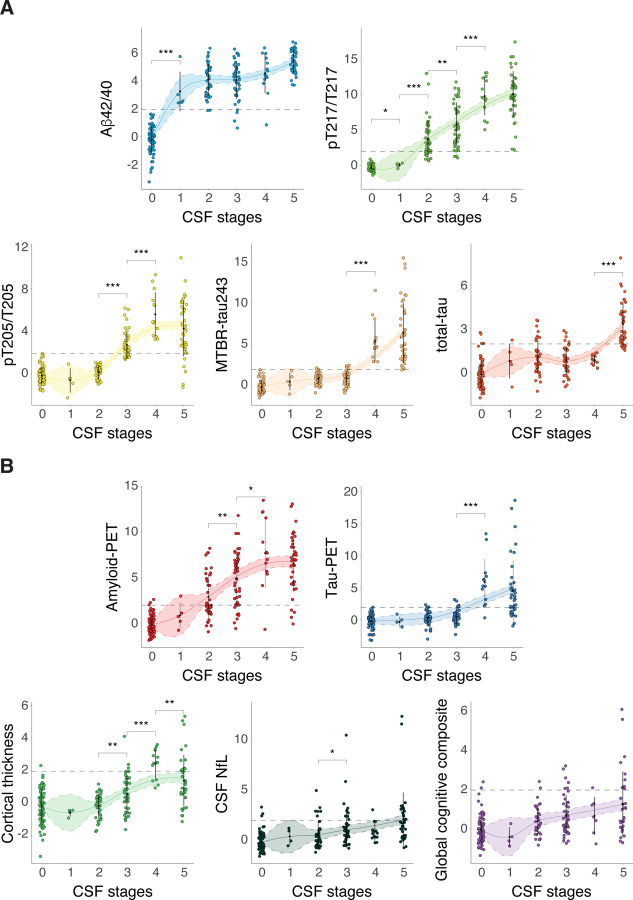
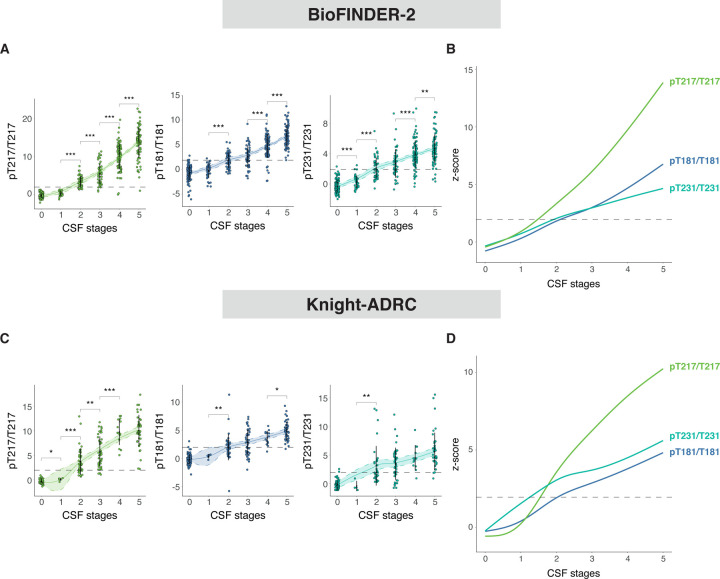
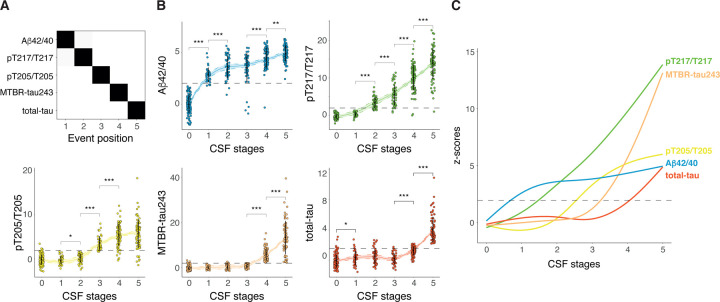
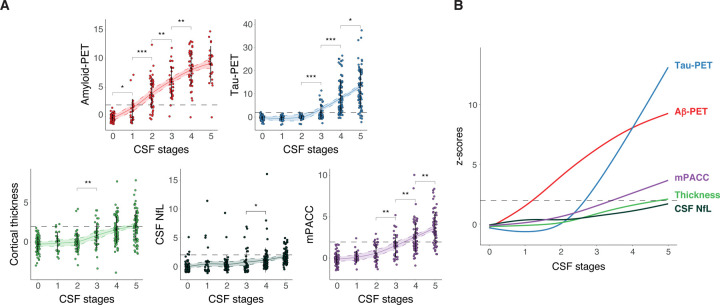
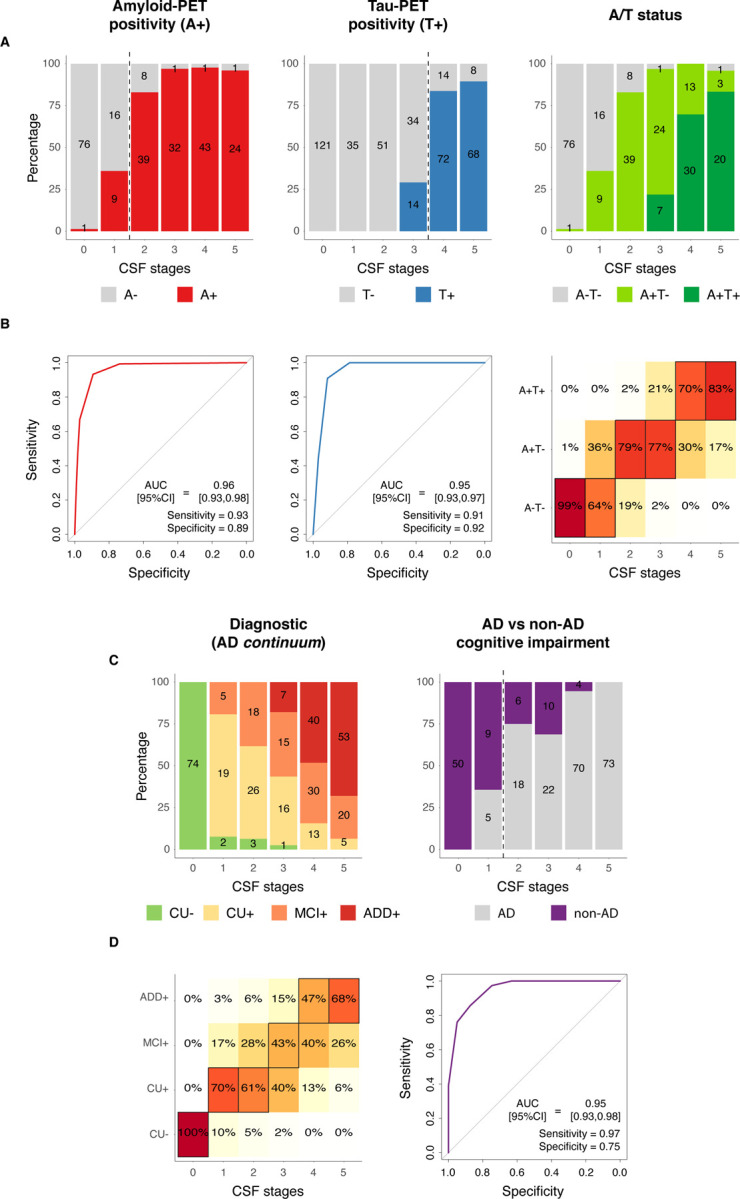
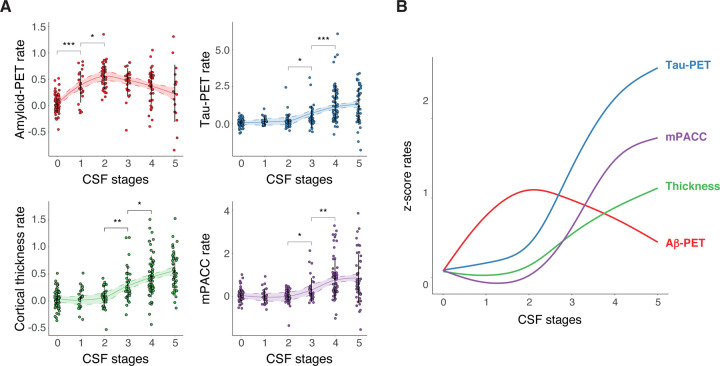
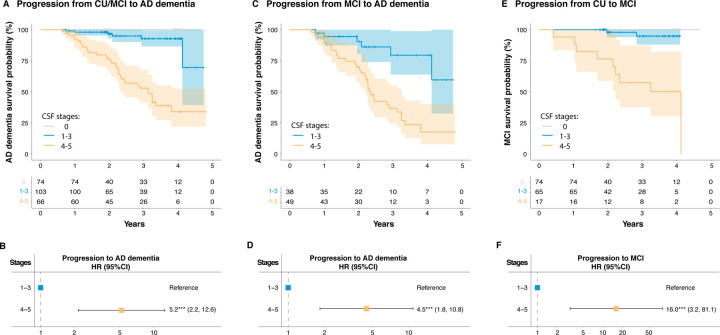
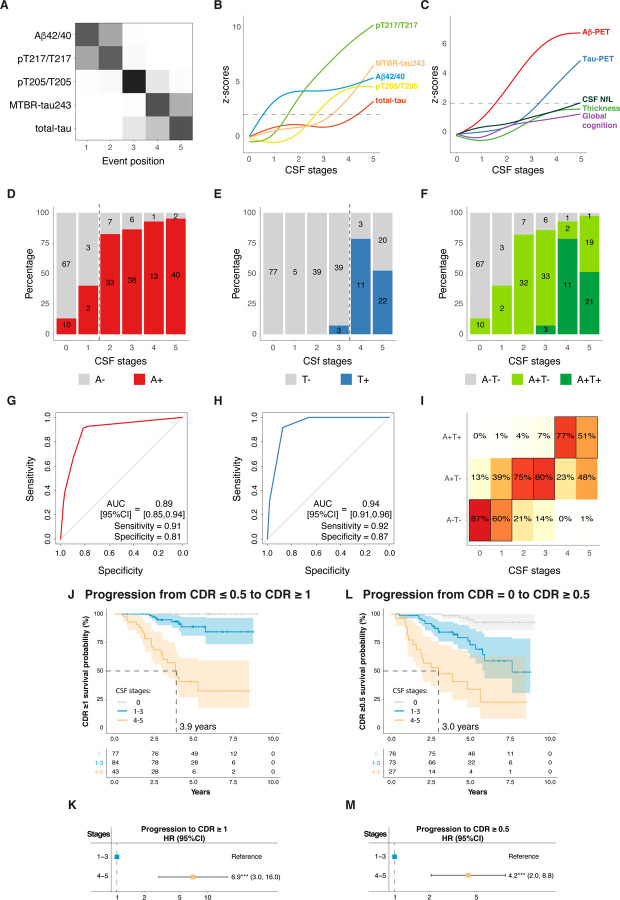
Biological staging of individuals with Alzheimer's disease (AD) may improve diagnostic and prognostic work-up of dementia in clinical practice and the design of clinical trials. Here, we created a staging model using the Subtype and Stage Inference (SuStaIn) algorithm by evaluating cerebrospinal fluid (CSF) amyloid-β (Aβ) and tau biomarkers in 426 participants from BioFINDER-2, that represent the entire spectrum of AD. The model composition and main analyses were replicated in 222 participants from the Knight ADRC cohort. SuStaIn revealed in the two cohorts that the data was best explained by a single biomarker sequence (one subtype), and that five CSF biomarkers (ordered: Aβ42/40, tau phosphorylation occupancies at the residues 217 and 205 [pT217/T217 and pT205/T205], microtubule-binding region of tau containing the residue 243 [MTBR-tau243], and total tau) were sufficient to create an accurate disease staging model. Increasing CSF stages (0-5) were associated with increased abnormality in other AD-related biomarkers, such as Aβ- and tau-PET, and aligned with different phases of longitudinal biomarker changes consistent with current models of AD progression. Higher CSF stages at baseline were associated with higher hazard ratio of clinical decline. Our findings indicate that a common pathophysiologic molecular pathway develops across all AD patients, and that a single CSF collection is sufficient to reliably indicate the presence of both AD pathologies and the degree and stage of disease progression.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources