

Temporal genomic heterogeneity guiding individualized therapy in recurrent non-small cell lung cancer
- PMID: 37503313
- PMCID: PMC10368968
- DOI: 10.3389/fonc.2023.1116809
Temporal genomic heterogeneity guiding individualized therapy in recurrent non-small cell lung cancer
Abstract
Introduction: Despite the benefit of adjuvant systemic therapy for patients with resected non-small cell lung cancer (NSCLC), the risk of postoperative recurrence remains high. Our objective was to characterize temporal genetic heterogeneity between primary resected and recurrent tumors, and its impact on treatment outcomes.
Methods: In this study, next-generation sequencing (NGS) testing was performed on tissue specimens and circulating tumor DNA (ctDNA) collected at postoperative recurrence, and results were compared to the genotypes of initial surgical specimens.
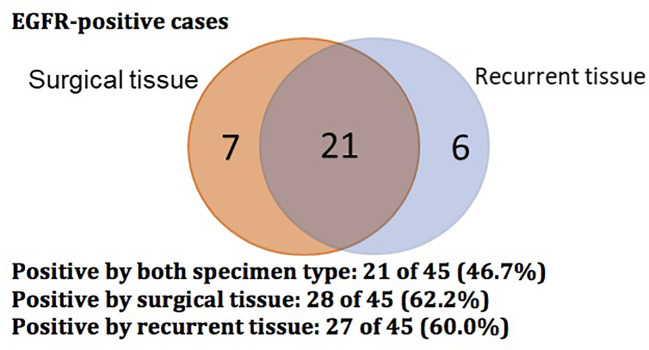
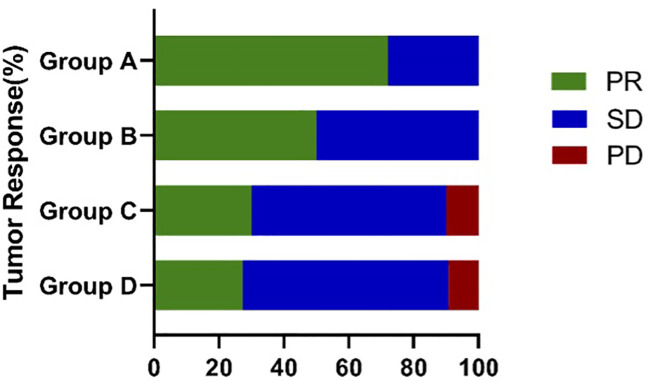
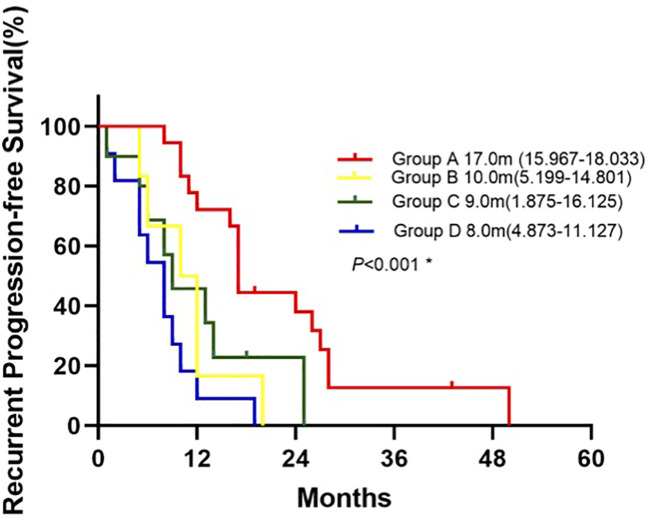
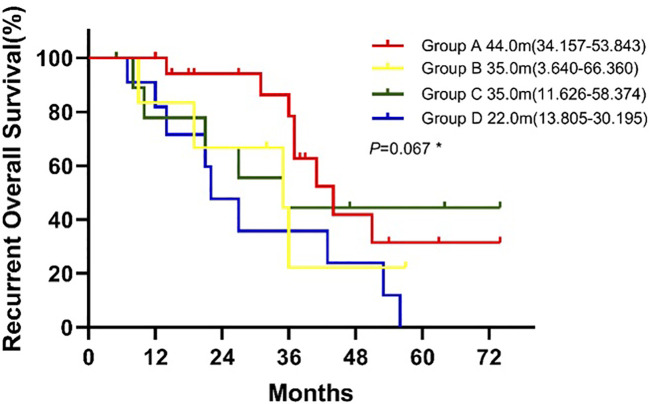
Results: Of forty-five patients with matched primary and post-operative recurrent tumors, EGFR status switched in 17 patients (37.8%) at post-operative recurrence and 28 patients (62.2%) had no genotype change (17 mutant, 11 wild-type). Based on the changes of EGFR status, patients were divided into 4 groups. Following subsequent treatment with EGFR TKI o chemotherapy: In group A, with sustained sensitive mutation, the percentage achieving partial response (PR) was the highest, at 72.2%, the median progression-free survival (PFS) was 17 months, and the median overall survival (OS) was 44.0 months respectively; In group B, with genotype changed from wild-type to mutant, 50% achieved PR, PFS was 10 months, and OS was 35 months; In group C, in which mutant status shifted to wild-type or new co-mutation emerged, the percentage achieving PR was 30%, PFS was 9 months, and OS was 35 months. In group D, with sustained wild type, the percentage achieving PR was 27.3%, PFS was 8 months, and OS was 22 months.
Discussion: Genotypic shift between paired primary and post-operative recurrent tumors was not infrequent, and this temporal genomic heterogeneity substantially impacted subsequent treatment outcomes.
Keywords: EGFR; NSCLC; dynamic gene sequencing; genotypic switch; temporal heterogeneity.
Copyright © 2023 Fang, Wan, D’Aiello, Sun, Gu, Li, Zhou, Xie, Deng, Cheng and Zhou.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
EGFR inhibitors as adjuvant therapy for resected non-small cell lung cancer harboring EGFR mutations.Lung Cancer. 2019 Oct;136:6-14. doi: 10.1016/j.lungcan.2019.08.001. Epub 2019 Aug 2. Lung Cancer. 2019. PMID: 31421260
-
Comprehensive characterization and clinical impact of concomitant genomic alterations in EGFR-mutant NSCLCs treated with EGFR kinase inhibitors.Lung Cancer. 2020 Jul;145:63-70. doi: 10.1016/j.lungcan.2020.04.004. Epub 2020 Apr 17. Lung Cancer. 2020. PMID: 32408134
-
Quantification of mutant alleles in circulating tumor DNA can predict survival in lung cancer.Oncotarget. 2016 Apr 12;7(15):20810-24. doi: 10.18632/oncotarget.8021. Oncotarget. 2016. PMID: 26989078 Free PMC article.
-
A high number of co-occurring genomic alterations detected by NGS is associated with worse clinical outcomes in advanced EGFR-mutant lung adenocarcinoma: Data from LATAM population.Lung Cancer. 2022 Dec;174:133-140. doi: 10.1016/j.lungcan.2022.11.002. Epub 2022 Nov 9. Lung Cancer. 2022. PMID: 36379126
-
Effect of smoking status on progression-free and overall survival in non-small cell lung cancer patients receiving erlotinib or gefitinib: a meta-analysis.J Clin Pharm Ther. 2015 Dec;40(6):661-71. doi: 10.1111/jcpt.12332. Epub 2015 Nov 17. J Clin Pharm Ther. 2015. PMID: 26573867
Cited by
-
Optimizing Osimertinib for NSCLC: Targeting Resistance and Exploring Combination Therapeutics.Cancers (Basel). 2025 Jan 29;17(3):459. doi: 10.3390/cancers17030459. Cancers (Basel). 2025. PMID: 39941826 Free PMC article. Review.
-
Potential supplementary tumor markers for liquid biopsy in non-small cell lung cancer.Exp Biol Med (Maywood). 2025 May 29;250:10523. doi: 10.3389/ebm.2025.10523. eCollection 2025. Exp Biol Med (Maywood). 2025. PMID: 40510243 Free PMC article.
-
Therapeutic insights into epidermal growth factor receptor/reactive oxygen species proto-oncogene 1-receptor co-mutated non-small cell lung cancer: Crizotinib as a promising option.World J Clin Oncol. 2025 Mar 24;16(3):103297. doi: 10.5306/wjco.v16.i3.103297. World J Clin Oncol. 2025. PMID: 40130054 Free PMC article.
References
-
- Yamazaki K, Sugio K, Yamanaka T, Hirai F, Osoegawa A, Tagawa T, et al. . Prognostic factors in non-small cell lung cancer patients with postoperative recurrence following third-generation chemotherapy. Anticancer Res (2010) 30(4):1311–5. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous