

Parameters Governing the Fate of Fracture Fixation With Proximal Femoral Nailing (PFN) for Intertrochanteric Femur Fractures
- PMID: 37503460
- PMCID: PMC10368960
- DOI: 10.7759/cureus.40952
Parameters Governing the Fate of Fracture Fixation With Proximal Femoral Nailing (PFN) for Intertrochanteric Femur Fractures
Abstract
Introduction: A high mortality rate is associated with hip fractures in the elderly. This is because their bones are osteoporotic with implants having less hold and there are more co-morbidities associated with the elderly. Osteosynthesis with the proximal femoral nail (PFN) features the advantages of high rotational stability of the head-neck fragment. However, the use of the nail is technically ambitious and is accompanied by some risks of error, which can lead to failure. This study aims to understand the technical difficulties related to PFN and methods to mitigate them and radiological indicators for successful outcomes of PFN.
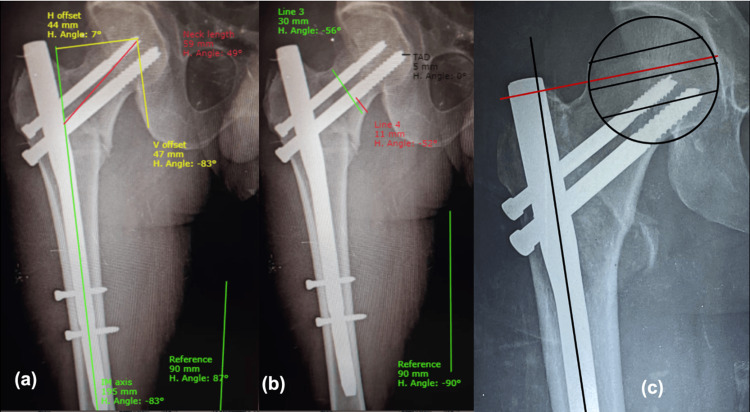
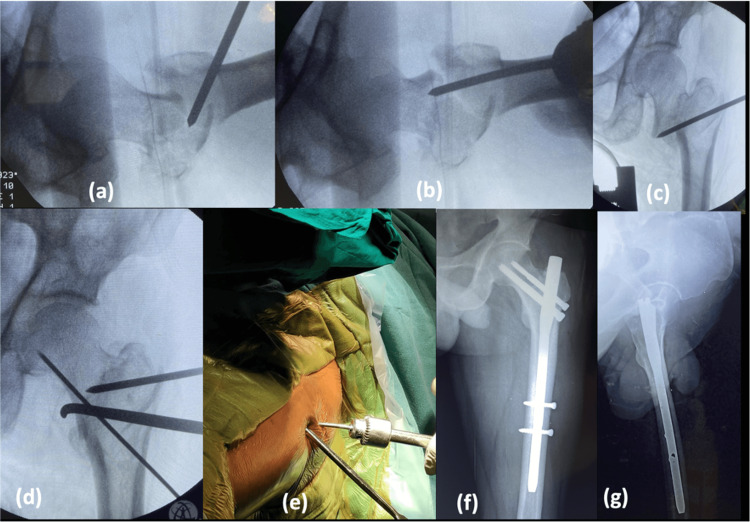
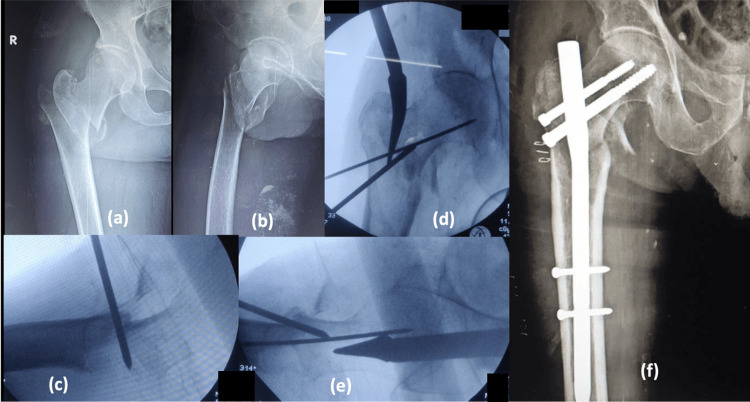
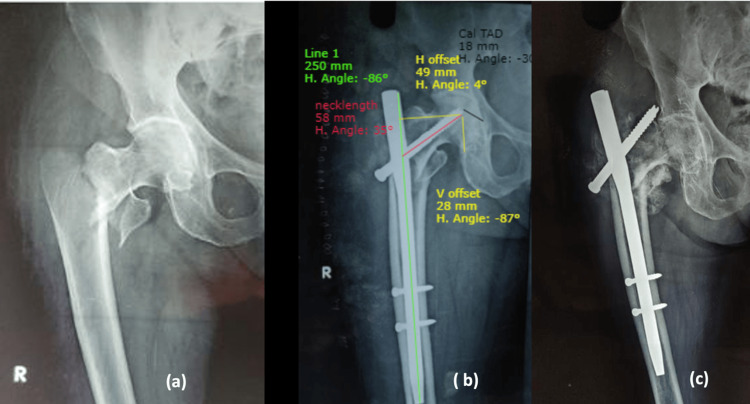
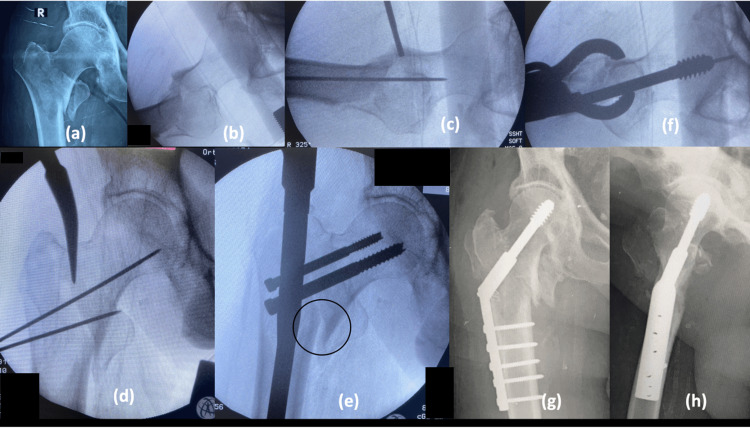
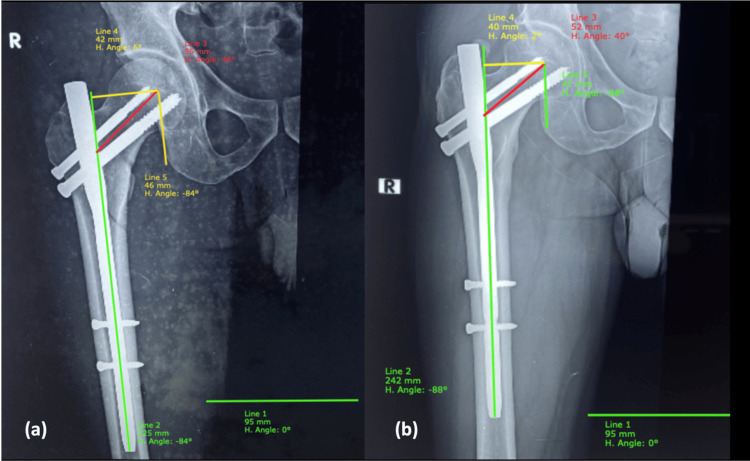
Methods: Our study aims to analyze the radiological parameters as indicators for the successful outcome of intertrochanteric fractures fixed using PFN and also the factors responsible for intraoperative conversion to dynamic hip screw (DHS). This is a prospective, observational study conducted from January 2020 to December 2020, on all the patients with intertrochanteric fractures who were planned to be treated by PFN and consented to be part of the study group at our institute. This study includes 99 cases of intertrochanteric fractures classified according to AO (Arbeitsgemeinschaft für Osteosynthesefragen)/Association of the Study of Internal Fixation (ASIF) and Evan's classification systems and followed postoperatively at regular intervals up to one year. Different methods of fracture reduction, intraoperative radiological parameters, and postoperative radiological parameters dictating the fate of PFN along with factors responsible for the intraoperative conversion to DHS were analyzed and discussed.
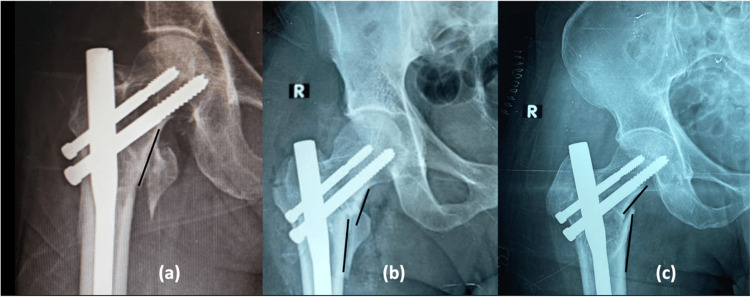
Results: Out of 99 patients planned for PFN, four were converted to DHS intraoperatively and 15 patients expired within the follow-up period of one year, leaving only 80 patients in the study group. Of them, seven patients (11.4%) had implant-related complications. According to Chang's reduction quality criteria (CRQC), two cases have CRQC 1 (poor reduction), 11 cases have CRQC 2 (acceptable reduction), 39 cases have CRQC 3 (acceptable reduction), and 28 cases have CRQC 4 (excellent reduction).
Conclusions: Though PFN is technically challenging, with proper guidelines and technique, it gives excellent results. Most importantly, a nonvarus reduction, proper nail insertion and accurate placement of lag screws are the crucial factors for a successful outcome. Biomechanically stable reduction, by closed, percutaneous, or open means, is the key to treating unstable intertrochanteric fracture successfully.
Keywords: chang’s reduction quality criteria; greater trochanter orthogonal line; hip offset; intertrochanteric fractures; intertrochanteric translation; parameters of pfn; parker's ratio; proximal femoral nail.
Copyright © 2023, Kund et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Evaluation of Functional and Radiological Outcome of Different Cephalomedullary Nail Designs in Intertrochanteric Fractures of Femur.J Orthop Case Rep. 2025 Mar;15(3):244-249. doi: 10.13107/jocr.2025.v15.i03.5402. J Orthop Case Rep. 2025. PMID: 40092258 Free PMC article.
-
Comparative study of intertrochanteric fracture fixation using proximal femoral nail with and without distal interlocking screws.World J Orthop. 2022 Mar 18;13(3):267-277. doi: 10.5312/wjo.v13.i3.267. eCollection 2022 Mar 18. World J Orthop. 2022. PMID: 35317250 Free PMC article.
-
Comparison of radiological and functional outcome of unstable intertrochanteric femur fractures treated using PFN and PFNA-2 in patients with osteoporosis.Eur J Orthop Surg Traumatol. 2019 Jul;29(5):1035-1042. doi: 10.1007/s00590-019-02401-x. Epub 2019 Feb 18. Eur J Orthop Surg Traumatol. 2019. PMID: 30778679
-
Proximal femoral nailing is superior to hemiarthroplasty in AO/OTA A2 and A3 intertrochanteric femur fractures in the elderly: a systematic literature review and meta-analysis.Int Orthop. 2020 Apr;44(4):623-633. doi: 10.1007/s00264-019-04351-9. Epub 2019 Jun 14. Int Orthop. 2020. PMID: 31201487
-
[Trochanteric femoral fractures].Acta Chir Orthop Traumatol Cech. 2013;80(1):15-26. Acta Chir Orthop Traumatol Cech. 2013. PMID: 23452417 Review. Czech.
Cited by
-
Design innovation and rationale of the intramedullary implants for treating Intertrochanteric fractures: A review.J Clin Orthop Trauma. 2024 Aug 30;56:102525. doi: 10.1016/j.jcot.2024.102525. eCollection 2024 Sep. J Clin Orthop Trauma. 2024. PMID: 39324022
References
-
- Type II intertrochanteric fractures: proximal femoral nailing (PFN) versus dynamic hip screw (DHS) Jonnes C, Shishir SM, Najimudeen S. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4733231/ Arch Bone Jt Surg. 2016;4:23–28. - PMC - PubMed
-
- Predictors of cut-out after cephalomedullary nail fixation of pertrochanteric fractures: a retrospective study of 813 patients. Murena L, Moretti A, Meo F, Saggioro E, Barbati G, Ratti C, Canton G. Arch Orthop Trauma Surg. 2018;138:351–359. - PubMed
-
- The Harris hip score: comparison of patient self-report with surgeon assessment. Mahomed NN, Arndt DC, McGrory BJ, Harris WH. J Arthroplasty. 2001;16:575–580. - PubMed
LinkOut - more resources
Full Text Sources