

The Importance of Awaiting Biopsy Results in Solitary Pathological Proximal Femoral Fractures : Do We Need to Biopsy Solitary Pathological Fractures?
- PMID: 37505350
- PMCID: PMC10562502
- DOI: 10.1245/s10434-023-13931-4
The Importance of Awaiting Biopsy Results in Solitary Pathological Proximal Femoral Fractures : Do We Need to Biopsy Solitary Pathological Fractures?
Abstract
Background: The optimal surgical treatment for patients presenting with (impending and complete) pathological proximal femoral fractures is predicated on prognosis. Guidelines recommend a preoperative biopsy to exclude sarcomas, however no evidence confirms a benefit.
Objective: This study aimed to describe the diagnostic accuracy, morbidity and sarcoma incidence of biopsy results in these patients.
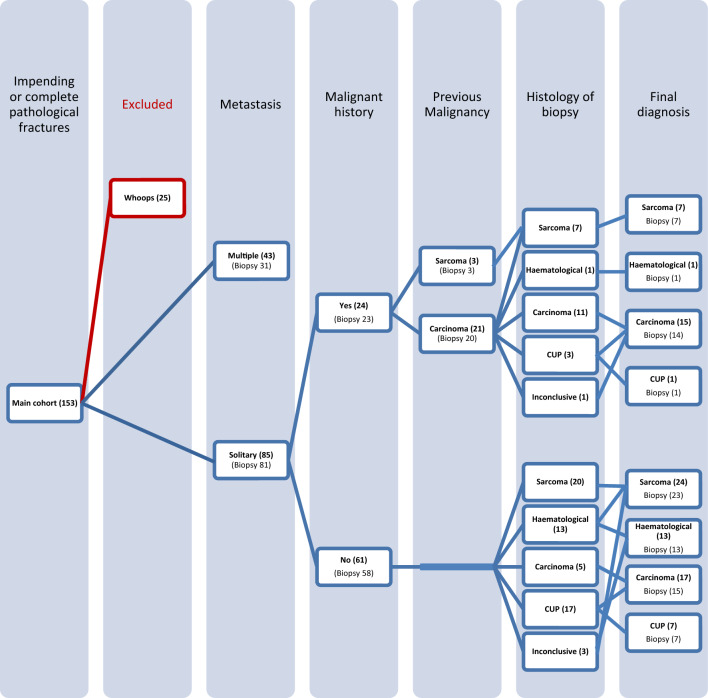
Material and methods: All patients (n = 153) presenting with pathological proximal femoral fractures between 2000 and 2019 were retrospectively evaluated. Patients after inadvertent surgery (n = 25) were excluded. Descriptive statistics were used to evaluate the accuracy and morbidity of diagnostic biopsies.
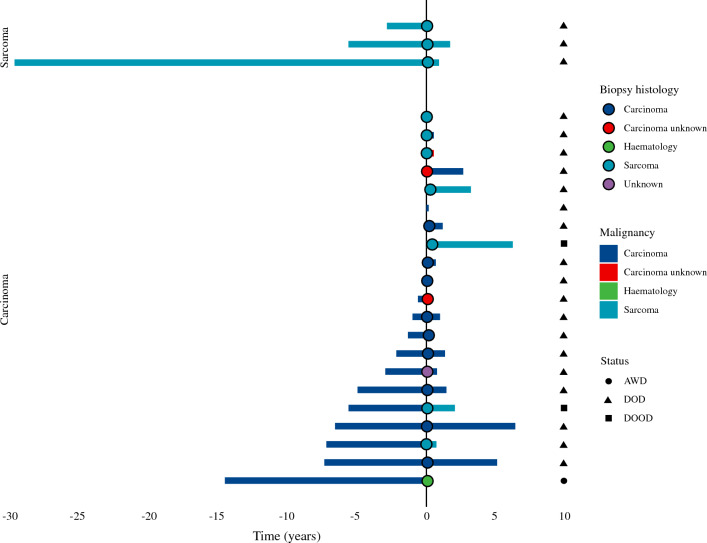
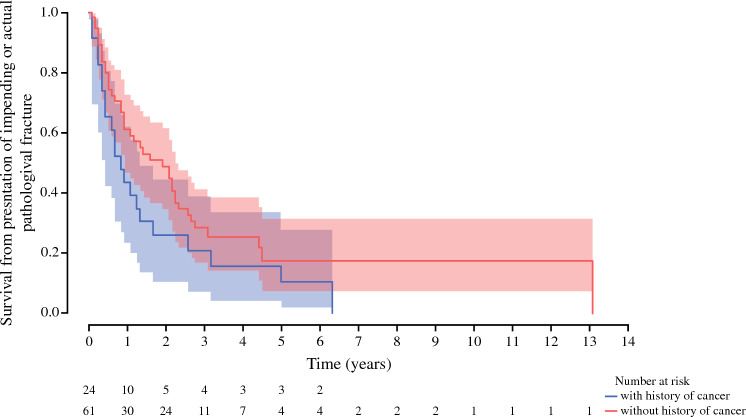
Results: Of 112/128 patients who underwent biopsy, nine (8%) biopsies were unreliable either due to being inconclusive (n = 5) or because the diagnosis changed after resection (n = 4). Of impending fractures, 32% fractured following needle core biopsy. Median time from diagnosis to surgery was 30 days (interquartile range 21-46). The overall biopsy positive predictive value (PPV) to differentiate between sarcoma and non-sarcoma was 1.00 (95% confidence interval [CI] 0.88-1.00). In patients with a previous malignancy (n = 24), biopsy (n = 23) identified the diagnosis in 83% (PPV 0.91, 95% CI 0.71-0.99), of whom five (24%) patients had a new diagnosis. In patients without a history of cancer (n = 61), final diagnosis included carcinomas (n = 24, 39.3%), sarcomas (n = 24, 39.3%), or hematological malignancies (n = 13, 21.3%). Biopsy (n = 58) correctly identified the diagnosis in 66% of patients (PPV 0.80, 95% CI 0.67-0.90).
Conclusion: This study confirms the importance of a preoperative biopsy in solitary pathological proximal femoral fractures due to the risk of sarcoma in patients with and without a history of cancer. However, biopsy delays the time to definite surgery, results can be inconclusive or false, and it risks completion of impending fractures.
© 2023. The Author(s).
Conflict of interest statement
Floortje G.M. Verspoor, Gerjon Hannink, Michael Parry, Lee Jeys, and Jonathan D. Stevenson have no conflicts of interest to declare.
Figures
References
-
- PH E. Cancer in the West Midlands. 2017.
LinkOut - more resources
Full Text Sources
