

Race-Specific Spirometry Equations Do Not Improve Models of Dyspnea and Quantitative Chest CT Phenotypes
- PMID: 37507005
- PMCID: PMC10925545
- DOI: 10.1016/j.chest.2023.07.019
Race-Specific Spirometry Equations Do Not Improve Models of Dyspnea and Quantitative Chest CT Phenotypes
Abstract
Background: Race-specific spirometry reference equations are used globally to interpret lung function for clinical, research, and occupational purposes, but inclusion of race is under scrutiny.
Research question: Does including self-identified race in spirometry reference equation formation improve the ability of predicted FEV1 values to explain quantitative chest CT abnormalities, dyspnea, or Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification?
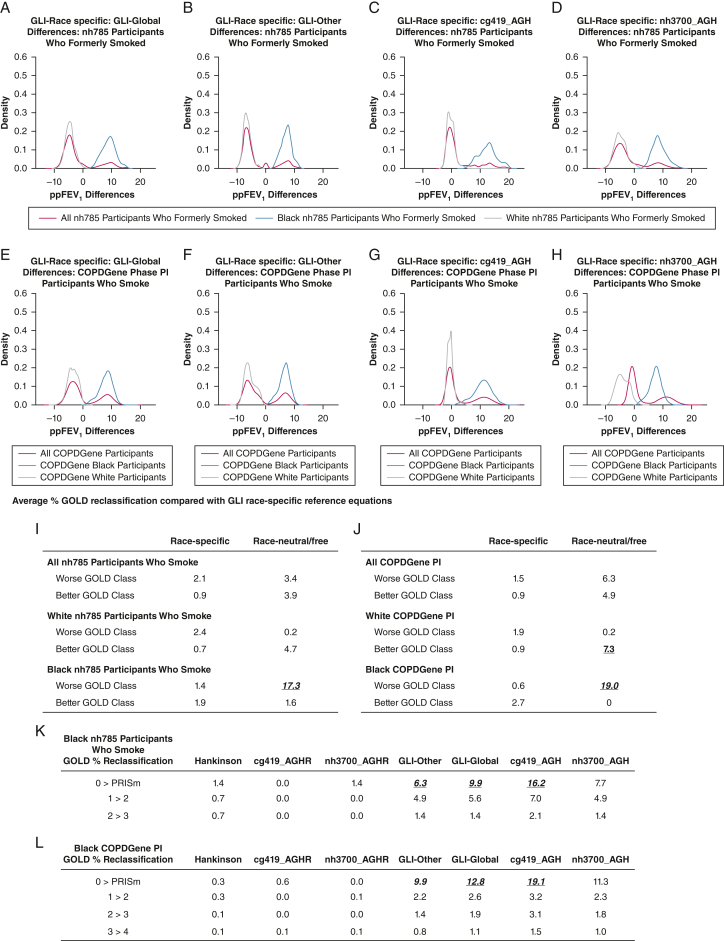
Study design and methods: Using data from healthy adults who have never smoked in both the National Health and Nutrition Survey (2007-2012) and COPDGene study cohorts, race-neutral, race-free, and race-specific prediction equations were generated for FEV1. Using sensitivity/specificity, multivariable logistic regression, and random forest models, these equations were applied in a cross-sectional analysis to populations of individuals who currently smoke and individuals who formerly smoked to determine how they affected GOLD classification and the fit of models predicting quantitative chest CT phenotypes or dyspnea.
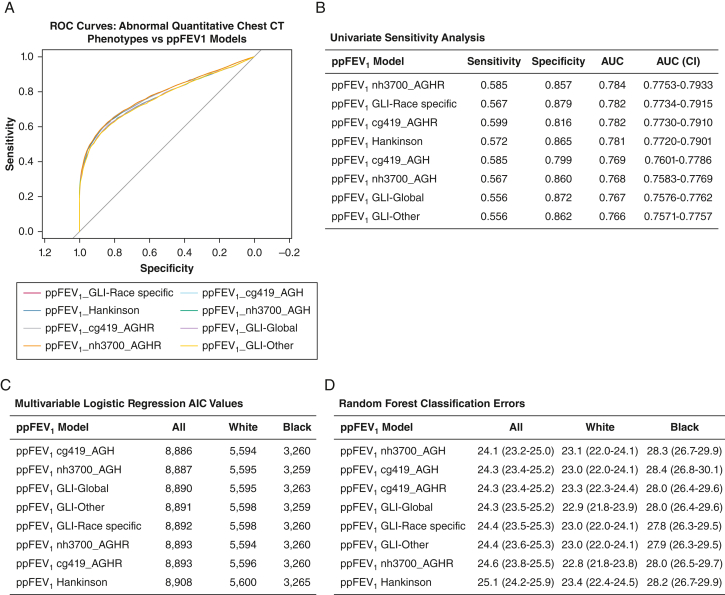
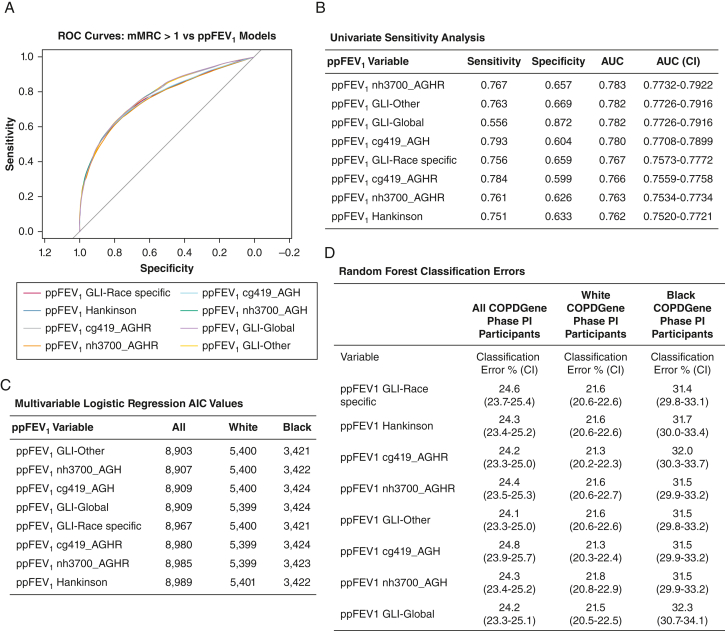
Results: Race-specific equations showed no advantage relative to race-neutral or race-free equations in models of quantitative chest CT phenotypes or dyspnea. Race-neutral reference equations reclassified up to 19% of Black participants into more severe GOLD classes, while race-neutral/race-free equations may improve model fit for dyspnea symptoms relative to race-specific equations.
Interpretation: Race-specific equations offered no advantage over race-neutral/race-free equations in three distinct explanatory models of dyspnea and chest CT scan abnormalities. Race-neutral/race-free reference equations may improve pulmonary disease diagnoses and treatment in populations highly vulnerable to lung disease.
Keywords: ethnicity; pulmonary function test; race; reference equations; spirometry.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Financial/Nonfinancial Disclosures The authors have reported to CHEST the following: A. L. N. receives support from UCSD Academic Senate and UCSD Division of Social Sciences Research grants. A. A. D. declares speaker fees from Boehringer Ingelheim, outside of the submitted work. A. K. B. is funded by the National Institutes of Health (NIH) [Grants KL2TR002492 and UL1TR002494], unrelated to the current work. S. P. B. is supported by the NIH [Grants R01 HL151421 and NIH UH3HL155806], Nuvaira, and Sanofi; and has received royalties from Springer Humana and consulting fees from Boehringer Ingelheim, Sanofi/Regeneron, and IntegrityCE, unrelated to the current work. R. C. has been supported by grants from AstraZeneca, Regeneron, and Genentech; consulting fees from Regeneron, Genentech, Inogen, and Boehringer Ingelheim; and honoraria from GlaxoSmithKline, unrelated to current work. R. C. is also on the Board of Directors for the COPD Foundation and President of the Pulmonary Education and Research Foundation. None declared (B. B., E. A. R., A. W., A. L., C. R., G. K., K. A. Y., B. F., C. H., D. J. C.).
Figures

Comment in
-
The Race to Abandon Ethnicity in Interpreting Pulmonary Function: Further Evidence.Chest. 2023 Dec;164(6):1348-1349. doi: 10.1016/j.chest.2023.08.022. Chest. 2023. PMID: 38070955 No abstract available.
References
-
- Hankinson J.L., Odencrantz J.R., Fedan K.B. Spirometric reference values from a sample of the general US population. Am J Respir Crit Care Med. 1999;159(1):179–187. - PubMed
-
- Braun L. University of Minnesota Press; Minneapolis, MN: 2014. Breathing Race into the Machine: The Surprising Career of the Spirometer from Plantation to Genetics.
