

A small area model to assess temporal trends and sub-national disparities in healthcare quality
- PMID: 37507373
- PMCID: PMC10382513
- DOI: 10.1038/s41467-023-40234-9
A small area model to assess temporal trends and sub-national disparities in healthcare quality
Abstract
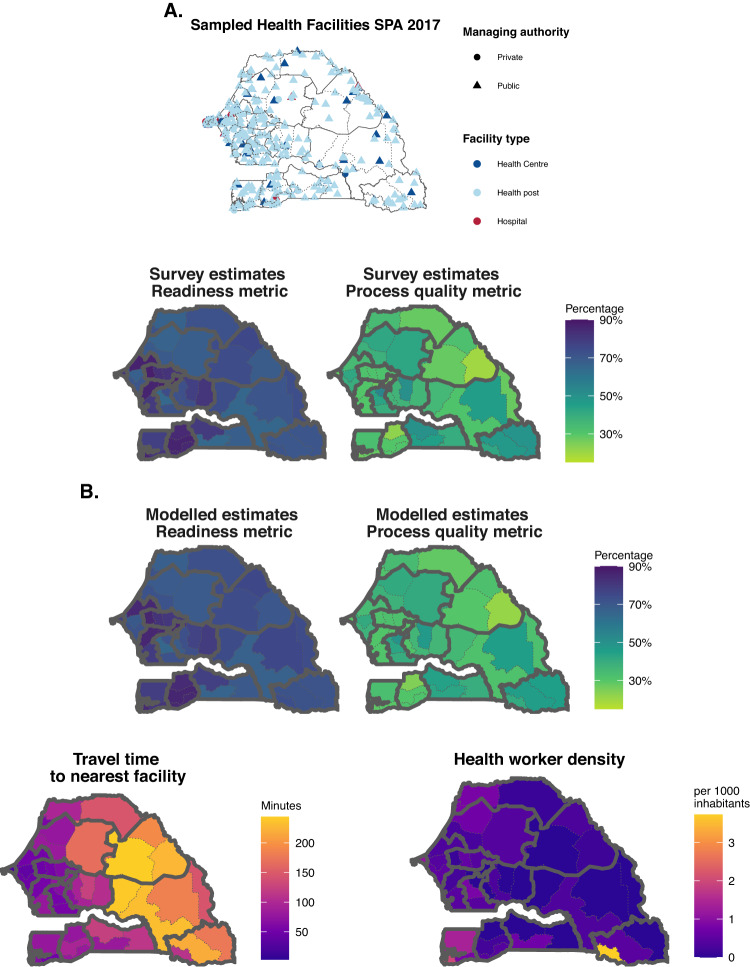
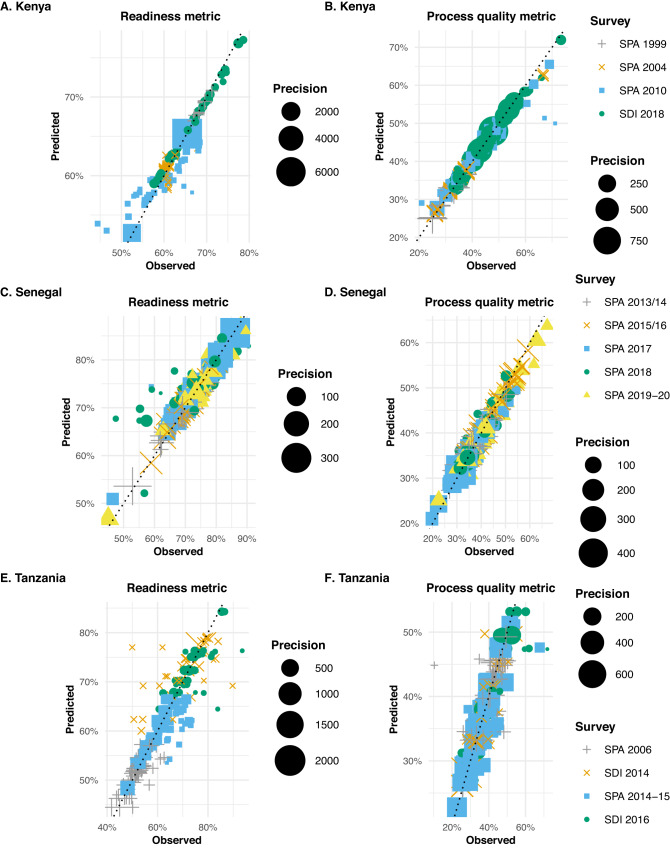
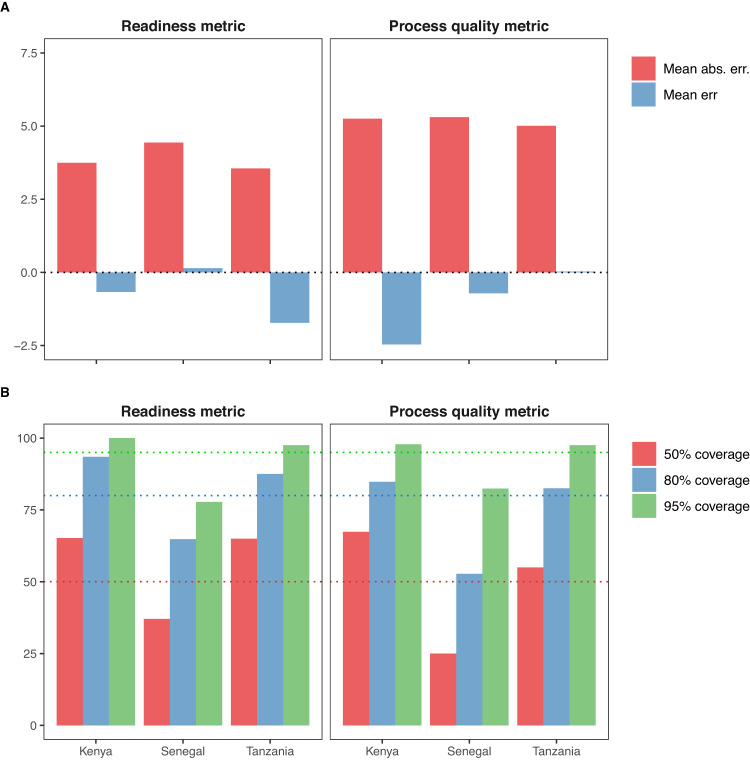
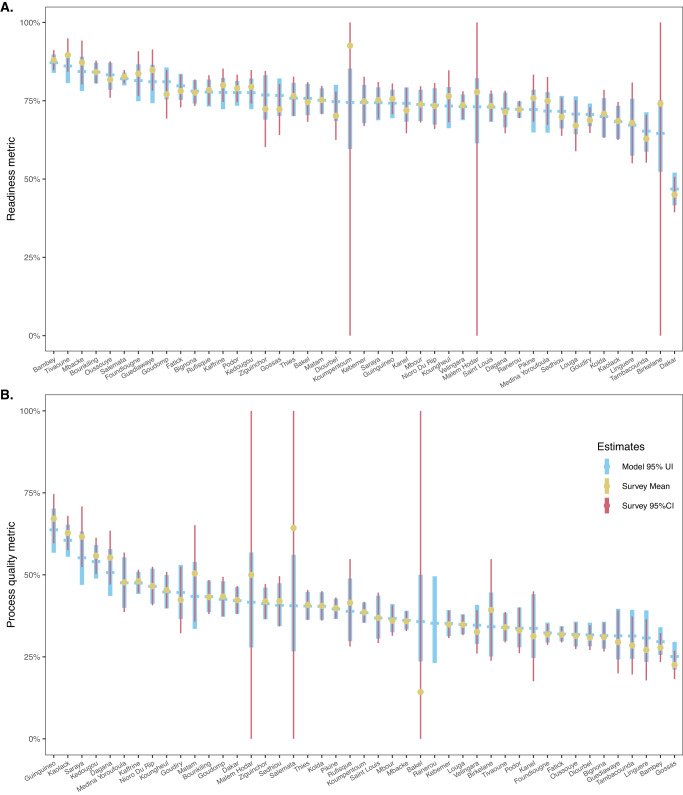
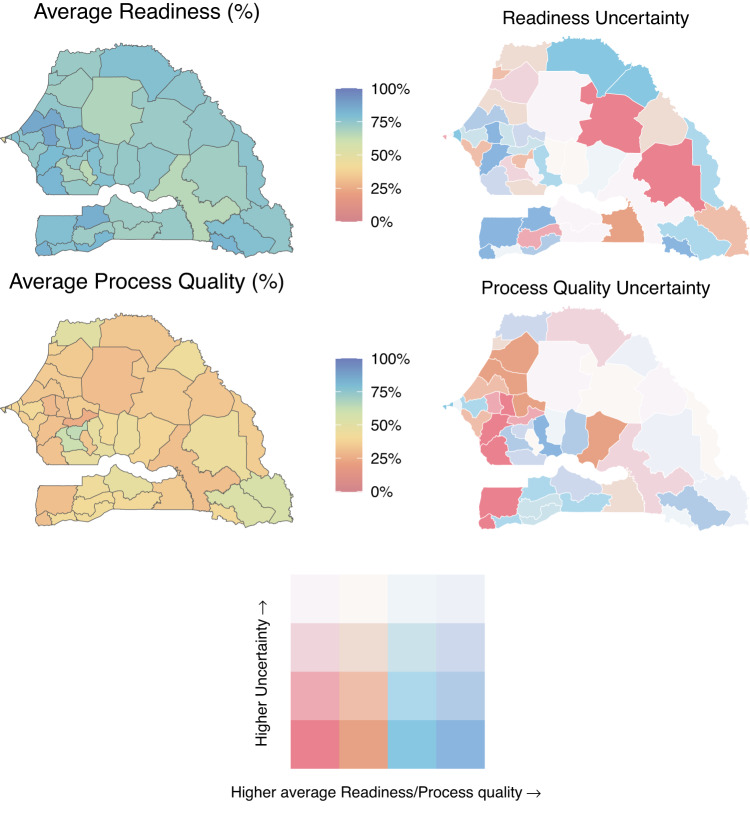
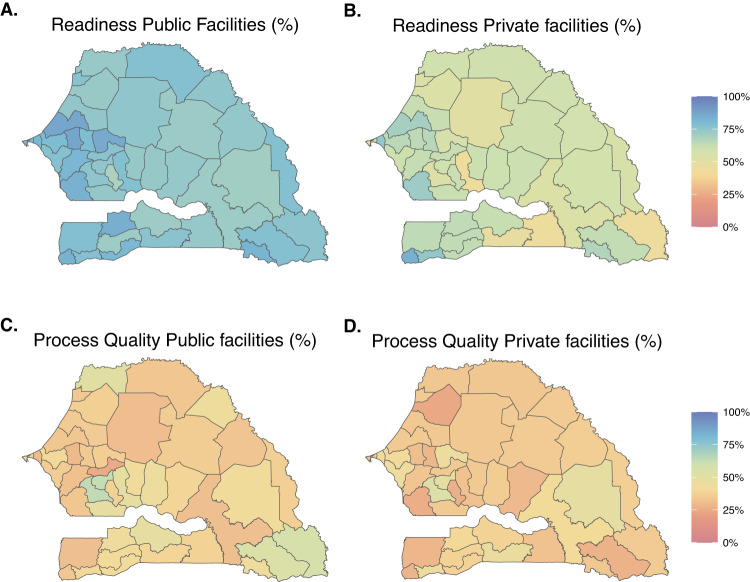
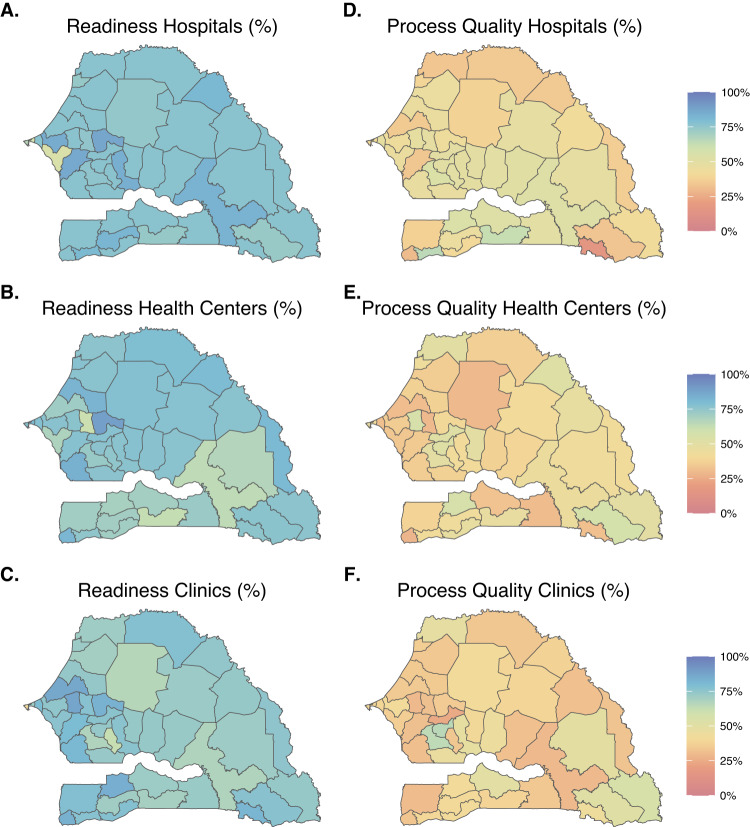
Monitoring subnational healthcare quality is important for identifying and addressing geographic inequities. Yet, health facility surveys are rarely powered to support the generation of estimates at more local levels. With this study, we propose an analytical approach for estimating both temporal and subnational patterns of healthcare quality indicators from health facility survey data. This method uses random effects to account for differences between survey instruments; space-time processes to leverage correlations in space and time; and covariates to incorporate auxiliary information. We applied this method for three countries in which at least four health facility surveys had been conducted since 1999 - Kenya, Senegal, and Tanzania - and estimated measures of sick-child care quality per WHO Service Availability and Readiness Assessment (SARA) guidelines at programmatic subnational level, between 1999 and 2020. Model performance metrics indicated good out-of-sample predictive validity, illustrating the potential utility of geospatial statistical models for health facility data. This method offers a way to jointly estimate indicators of healthcare quality over space and time, which could then provide insights to decision-makers and health service program managers.
© 2023. The Author(s).
Conflict of interest statement
N.F. reports financial support from Gates Ventures since June 2020 outside of the submitted work. All other authors declare no competing interests.
Figures
References
-
- United Nations, S. Global indicator framework for the Sustainable Development Goals and targets of the 2030 Agenda for Sustainable Development. (2017).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
