

MRI features of idiopathic intracranial hypertension are not prognostic of visual and headache outcome
- PMID: 37507663
- PMCID: PMC10386656
- DOI: 10.1186/s10194-023-01641-x
MRI features of idiopathic intracranial hypertension are not prognostic of visual and headache outcome
Abstract
Background: In idiopathic intracranial hypertension (IIH), certain MRI features are promising diagnostic markers, but whether these have prognostic value is currently unknown.
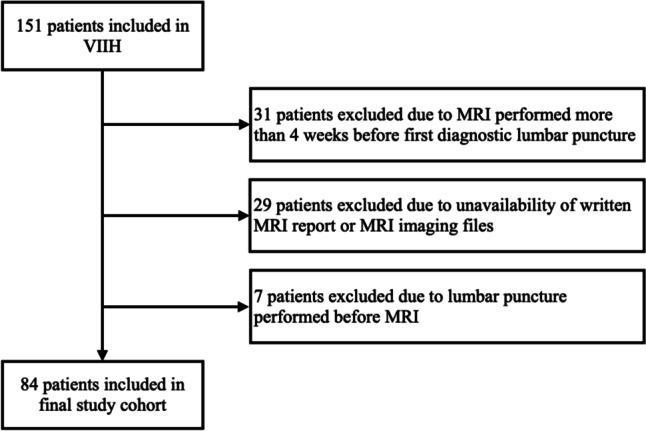
Methods: We included patients from the Vienna-Idiopathic-Intracranial-Hypertension (VIIH) database with IIH according to Friedman criteria and cranial MRI performed at diagnosis. Presence of empty sella (ES), perioptic subarachnoid space distension (POSD) with or without optic nerve tortuosity (ONT), posterior globe flattening (PGF) and transverse sinus stenosis (TSS) was assessed and multivariable regression models regarding visual outcome (persistent visual impairment/visual worsening) and headache outcome (headache improvement/freedom of headache) were fitted.
Results: We included 84 IIH patients (88.1% female, mean age 33.5 years, median body mass index 33.7). At baseline, visual impairment was present in 70.2% and headache in 84.5% (54.8% chronic). Persistent visual impairment occurred in 58.3%, visual worsening in 13.1%, headache improvement was achieved in 83.8%, freedom of headache in 26.2%. At least one MRI feature was found in 78.6% and 60.0% had ≥3 features with POSD most frequent (64.3%) followed by TSS (60.0%), ONT (46.4%), ES (44.0%) and PGF (23.8%). In multivariable models, there was no association of any single MRI feature or their number with visual impairment, visual worsening, headache improvement or freedom. Visual impairment at baseline predicted persistent visual impairment (odds ratio 6.3, p<0.001), but not visual worsening. Chronic headache at baseline was significantly associated with lower likelihood of headache freedom (odds ratio 0.48, p=0.013), but not with headache improvement.
Conclusions: MRI features of IIH are neither prognostic of visual nor headache outcome.
Keywords: Empty sella; Idiopathic intracranial hypertension; Magnetic resonance imaging; Optic nerve tortuosity; Perioptic subarachnoid space distension; Posterior globe flattening; Transverse sinus stenosis; Visual outcome.
© 2023. The Author(s).
Conflict of interest statement
GB: has participated in meetings sponsored by, received speaker honoraria or travel funding from Biogen, Celgene/BMS, Lilly, Merck, Novartis, Roche, Sanofi-Genzyme and Teva, and received honoraria for consulting Biogen, Celgene/BMS, Novartis, Roche, Sanofi-Genzyme and Teva. He has received unrestricted research grants from Celgene/BMS and Novartis. WM: declares no conflict of interest relevant to this study. SM: declares no conflict of interest relevant to this study. VS: declares no conflict of interest relevant to this study/ NK: has participated in meetings sponsored by, received speaker honoraria or travel funding from BMS/Celgene, Janssen-Cilag, Merck, Novartis, Roche and Sanofi-Genzyme and held a grant for a Multiple Sclerosis Clinical Training Fellowship Programme from the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS). PP: declares no conflict of interest relevant to this study. CM: declares no conflict of interest relevant to this study. KN: declares no conflict of interest relevant to this study. CW: has received honoraria consultancy/speaking from Apomedica, Curelator, Eli Lilly, Grünenthal, Hermes, Novartis, Pfizer, Ratiopharm/Teva, and Stada. BP: declares no conflict of interest relevant to this study.
Figures
References
-
- Radhakrishnan K, Ahlskog JE, Cross SA et al (1993) Idiopathic Intracranial Hypertension (Pseudotumor Cerebri): Descriptive Epidemiology in Rochester, Minn, 1976 to 1990. Arch Neurol-chicago 50(1):78–80 - PubMed
-
- Peng MG, Gokoffski KK. Updates on recent developments in idiopathic intracranial hypertension. SN Compr Clin Medicine. 2021;3:1031–1041. doi: 10.1007/s42399-021-00814-6. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
