

Clinical and imaging differences between Stanford Type B intramural hematoma-like lesions and classic aortic dissection
- PMID: 37507680
- PMCID: PMC10386763
- DOI: 10.1186/s12872-023-03413-6
Clinical and imaging differences between Stanford Type B intramural hematoma-like lesions and classic aortic dissection
Abstract
Background: Intramural hematoma (IMH) and Aortic dissection (AD) have overlapping features. The aim of this study was to explore the differences between them by comparing the clinical manifestations and imaging features of patients with acute Stanford type B IMH-like lesions and acute Stanford type B AD (ATBAD).
Methods: This study retrospectively analysed the clinical and computed tomography angiography (CTA) imaging data of 42 IMH-like lesions patients with ulcer-like projection (ULP) and 38 ATBAD patients, and compared their clinical and imaging features.
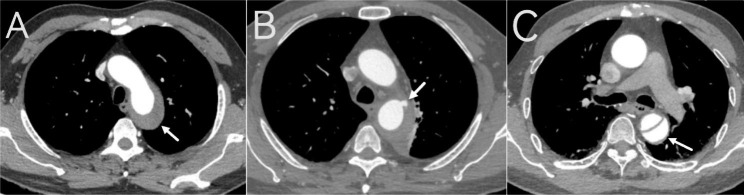
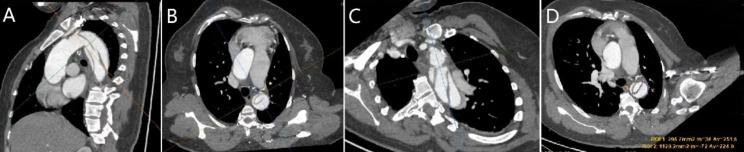
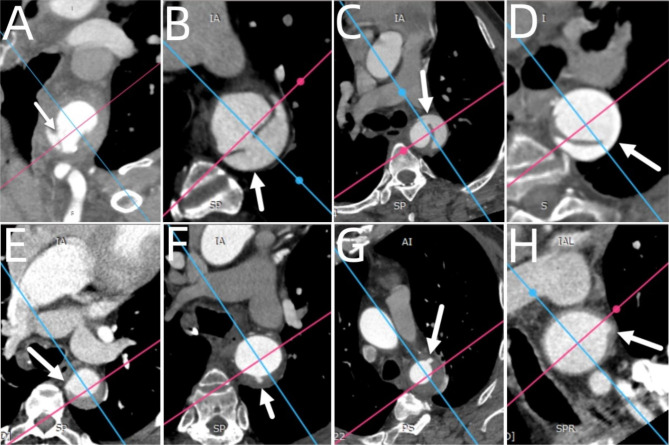
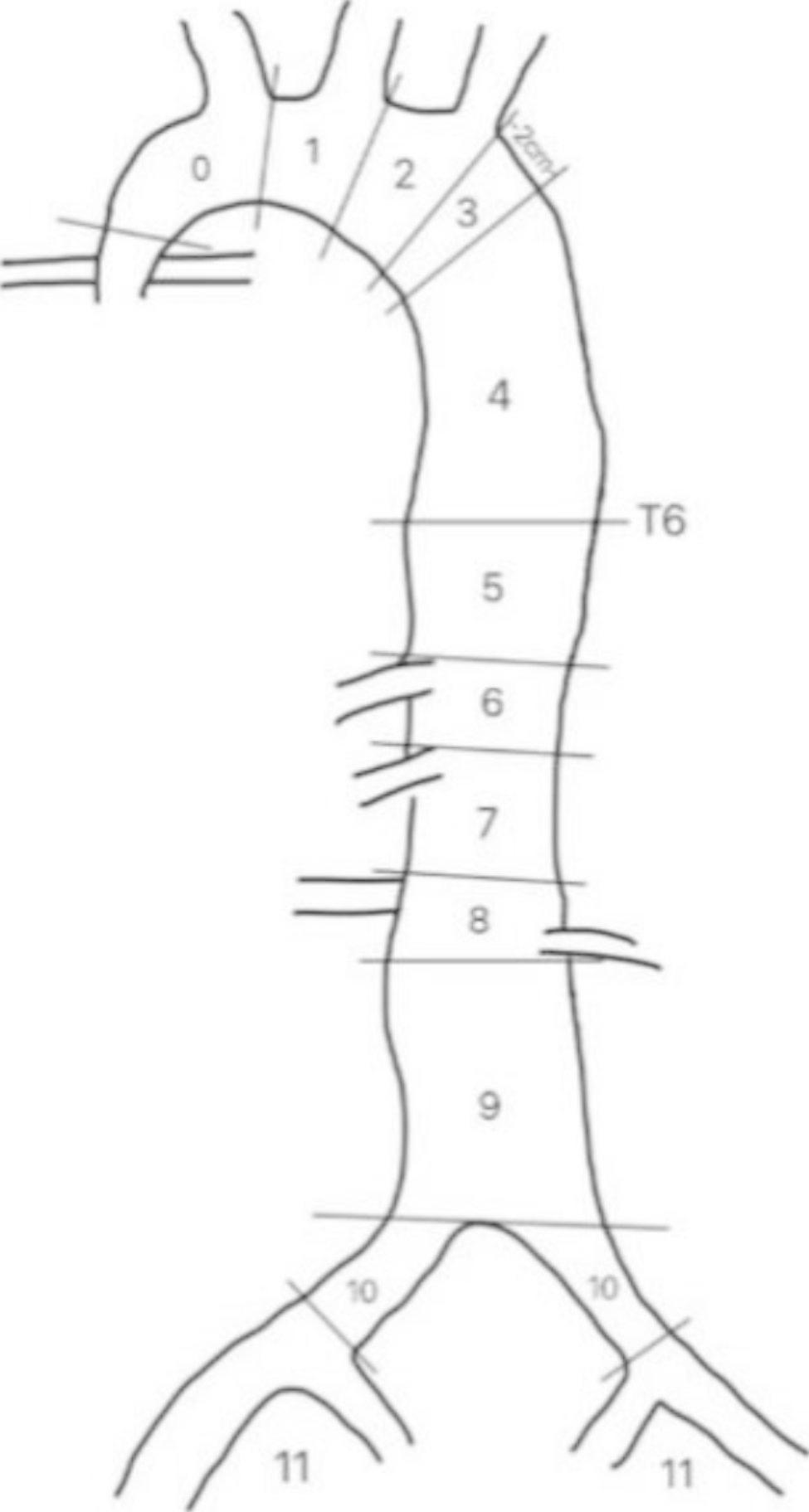
Results: (1) The IMH-like lesions patients were older than the ATBAD patients (64.2 ± 11.5 vs. 50.9 ± 12.2 years, P < 0.001). The D-dimer level in the IMH-like lesions group was significantly higher than that in the ATBAD group (11.2 ± 3.6 vs. 9.2 ± 4.5 mg/L, P < 0.05). The incidence rate of back pain was significantly higher in the ATBAD group than in the IMH-like lesions group (71.1% vs. 26.2%, P < 0.05). (2) The ULPs of IMH-like lesions and the intimal tears of ATBAD were concentrated in zone 4 of the descending thoracic aorta. The ULPs of IMH-like lesions and the intimal tears of ATBAD were mainly in the upper quadrant outside the lumen (64.3% vs. 65.8%, P > 0.05). (3) The maximum diameter of the ULPs in IMH-like lesions was smaller than that of the intimal tears in ATBAD (7.4 ± 3.4 vs. 10.8 ± 6.8 mm, P = 0.005). The lumen compression ratio in the ULPs plane and the maximum compression ratio of the aortic lumen in the IMH-like lesions group were smaller than that in the ADBAD group (P < 0.05). Fewer aortic segments were involved in IMH-like lesions patients than in ATBAD patients (5.6 ± 2.2 vs. 7.1 ± 1.9 segments, P < 0.005). The IMH-like lesions group had less branch involvement than that of the ATBAD group (P < 0.001).
Conclusion: The degree of intimal tears, lumen compression ratio, extent of lesion involvement, and impact on branch arteries in ATBAD are more severe than that of IMH-like lesions. But for the ULPs of IMH-like lesions and intimal tears of ATBAD, they have astonishing similarities in the location of the partition and the lumen quadrant, we have reason to believe that intimal tear is the initial factor in the pathogenesis of this kind of disease, and their clinical and imaging manifestations overlap, but the severity is different. Concerning similarities between these two conditions, these two may be a spectrum of one disease.
Keywords: Acute aortic syndrome; CT angiography; IMH-like lesions; Intramural hematoma.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
An analysis of initial and follow-up CT findings in intramural hematoma, aortic double-lumen dissection, and mixed type lesions.Acta Radiol. 2015 Sep;56(9):1091-9. doi: 10.1177/0284185114549824. Epub 2014 Sep 26. Acta Radiol. 2015. PMID: 25260419
-
Pathologic variants of thoracic aortic dissections. Penetrating atherosclerotic ulcers and intramural hematomas.Cardiol Clin. 1999 Nov;17(4):637-57. doi: 10.1016/s0733-8651(05)70106-5. Cardiol Clin. 1999. PMID: 10589337
-
Detection of the intimal tear in aortic dissection and ulcer-like projection in intramural hematoma: usefulness of full-phase retrospective ECG-gated CT angiography.Jpn J Radiol. 2020 Nov;38(11):1036-1045. doi: 10.1007/s11604-020-01008-1. Epub 2020 Jul 24. Jpn J Radiol. 2020. PMID: 32710132 Free PMC article.
-
Medical and surgical management of acute type B aortic intramural hematoma.J Card Surg. 2020 Sep;35(9):2324-2330. doi: 10.1111/jocs.14823. Epub 2020 Jul 15. J Card Surg. 2020. PMID: 32668075 Review.
-
Tailored treatment modality in acute type A intramural hematoma.J Thorac Cardiovasc Surg. 2023 Nov;166(5):1400-1410. doi: 10.1016/j.jtcvs.2022.01.037. Epub 2022 Feb 3. J Thorac Cardiovasc Surg. 2023. PMID: 35221028 Review.
Cited by
-
A nomogram prediction model for short-term aortic-related adverse events in patients with acute Stanford type B aortic intramural hematoma: development and validation.Front Cardiovasc Med. 2024 Jul 10;11:1364361. doi: 10.3389/fcvm.2024.1364361. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39049955 Free PMC article.
-
Prognosis prediction in type B aortic intramural hematoma patients using a combined model based on aortic computed tomography angiography radiomics.Quant Imaging Med Surg. 2025 Feb 1;15(2):1439-1454. doi: 10.21037/qims-24-1914. Epub 2025 Jan 22. Quant Imaging Med Surg. 2025. PMID: 39995707 Free PMC article.
-
CT diagnosis and destiny of acute aortic intramural hematoma.Front Radiol. 2025 Mar 11;5:1552644. doi: 10.3389/fradi.2025.1552644. eCollection 2025. Front Radiol. 2025. PMID: 40134989 Free PMC article. Review.
References
-
- Erbel R, Aboyans V, Boileau C, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the diagnosis and treatment of aortic Diseases of the European Society of Cardiology (ESC) [J] Eur Heart J. 2014;35(41):2873–926. doi: 10.1093/eurheartj/ehu281. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
