

Standardization and learning curve in laparoscopic hernia repair: experience of a high-volume center
- PMID: 37507714
- PMCID: PMC10385909
- DOI: 10.1186/s12893-023-02119-y
Standardization and learning curve in laparoscopic hernia repair: experience of a high-volume center
Abstract
Purpose: Groin hernias are a common condition that can be treated with various surgical techniques, including open surgery and laparoscopic approaches. Laparoscopic surgery has several advantages but its use is limited due to the complexity of the posterior inguinal region and the need for advanced laparoscopic skills. This paper presents a standardized and systematic approach to trans-abdominal pre-peritoneal (TAPP) groin hernioplasty, which is useful for training young surgeons.
Methods: The paper provides a detailed, step-by-step description of the TAPP based on evidence from literature, anatomical knowledge, and the authors' experience spanning over 30 years. The sample includes 487 hernia repair procedures, with 319 surgeries performed by experienced surgeons and 168 surgeries performed by young surgeons in training. The authors performed a descriptive analysis of their data to provide an overview of the volume of laparoscopic hernioplasty performed.
Results: The analysis of the data shows a low complication rate of 0.41% (2/487) and a low recurrence rate of 0.41% (2/487). The median duration of the surgery was 55 min, while the median operation time for surgeons in training was 93 min, specifically 83 min for unilateral hernia and 115 min for bilateral hernia.
Conclusions: The TAPP procedure appears, to date, comparable to the open inguinal approach in terms of recurrence, postoperative pain and speed of postoperative recovery. In this paper, the authors challenge the belief that TAPP is not suitable for surgeons in training. They advocate for a training pathway that involves gradually building surgical skills and expertise. This approach requires approximately 100 procedures to achieve proficiency.
Keywords: Critical view of safety; Groin hernia; Inguinal hernia; Laparoscopy; Mesh; TAPP; Transabdominal preperitoneal.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Kingsnorth A, LeBlanc K. ‘Hernias: inguinal and incisional’, The Lancet, vol. 362, no. 9395, pp. 1561–1571, Nov. 2003, 10.1016/S0140-6736(03)14746-0. - PubMed
-
- Fitzgibbons RJ et al. ‘Long-term Results of a Randomized Controlled Trial of a Nonoperative Strategy (Watchful Waiting) for Men With Minimally Symptomatic Inguinal Hernias’, Ann. Surg, vol. 258, no. 3, pp. 508–515, Sep. 2013, 10.1097/SLA.0b013e3182a19725. - PubMed
-
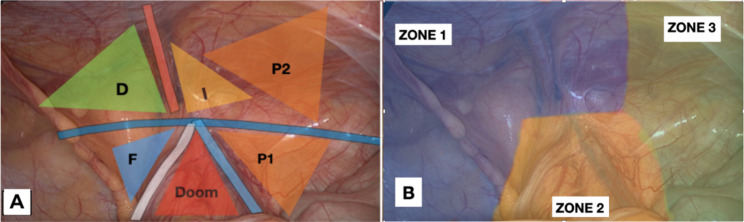
- Claus C, Furtado M, Malcher F, Cavazzola LT, Felix E. ‘Ten golden rules for a safe MIS inguinal hernia repair using a new anatomical concept as a guide’, Surg. Endosc, vol. 34, no. 4, pp. 1458–1464, Apr. 2020, 10.1007/s00464-020-07449-z. - PubMed
