

Elevated Copeptin Levels Are Associated with Heart Failure Severity and Adverse Outcomes in Children with Cardiomyopathy
- PMID: 37508636
- PMCID: PMC10377870
- DOI: 10.3390/children10071138
Elevated Copeptin Levels Are Associated with Heart Failure Severity and Adverse Outcomes in Children with Cardiomyopathy
Abstract
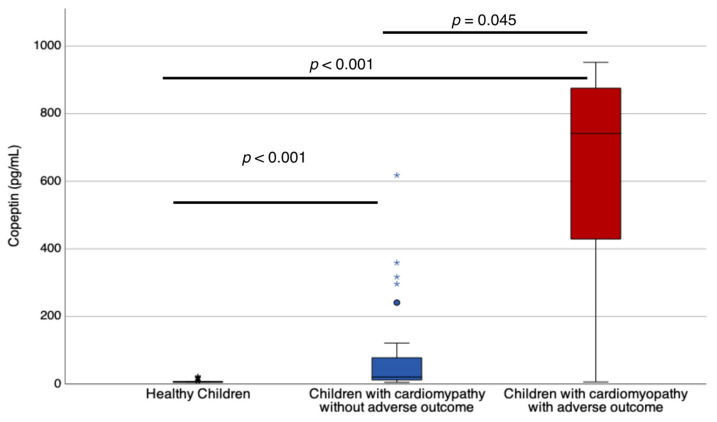
In children with cardiomyopathy, the severity of heart failure (HF) varies. However, copeptin, which is a biomarker of neurohormonal adaptation in heart failure, has not been studied in these patients. In this study, we evaluated the correlation of copeptin level with functional HF grading, B-type natriuretic peptide (BNP), and echocardiography variables in children with cardiomyopathy. Furthermore, we determined if copeptin levels are associated with adverse outcomes, including cardiac arrest, mechanical circulatory support, heart transplant, or death. In forty-two children with cardiomyopathy with a median (IQR) age of 13.1 years (2.5-17.2) and a median follow-up of 2.5 years (2.2-2.7), seven (16.7%) children had at least one adverse outcome. Copeptin levels were highest in the patients with adverse outcomes, followed by the patients without adverse outcomes, and then the healthy children. The copeptin levels in patients showed a strong correlation with their functional HF grading, BNP level, and left ventricular ejection fraction (LVEF). Patients with copeptin levels higher than the median value of 25 pg/mL had a higher likelihood of experiencing adverse outcomes, as revealed by Kaplan-Meier survival analysis (p = 0.024). Copeptin level was an excellent predictor of outcomes, with an area under the curve of 0.861 (95% CI, 0.634-1.089), a sensitivity of 86%, and a specificity of 60% for copeptin level of 25 pg/mL. This predictive value was superior in patients with dilated and restrictive cardiomyopathies (0.97 (CI 0.927-1.036), p < 0.0001, n = 21) than in those with hypertrophic and LV non-compaction cardiomyopathies (0.60 (CI 0.04-1.16), p = 0.7, n = 21).
Keywords: BNP; biomarkers; cardiomyopathy; copeptin; neurohormonal; pediatric heart failure.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures



References
-
- Rossano J.W., Kim J.J., Decker J.A., Price J.F., Zafar F., Graves D.E., Morales D.L., Heinle J.S., Bozkurt B., Towbin J.A., et al. Prevalence, morbidity, and mortality of heart failure-related hospitalization in the United States: A population-based study. J. Card. Fail. 2012;18:459–470. doi: 10.1016/j.cardfail.2012.03.001. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
