

Angiogenesis and Tissue Repair Depend on Platelet Dosing and Bioformulation Strategies Following Orthobiological Platelet-Rich Plasma Procedures: A Narrative Review
- PMID: 37509560
- PMCID: PMC10377284
- DOI: 10.3390/biomedicines11071922
Angiogenesis and Tissue Repair Depend on Platelet Dosing and Bioformulation Strategies Following Orthobiological Platelet-Rich Plasma Procedures: A Narrative Review
Abstract
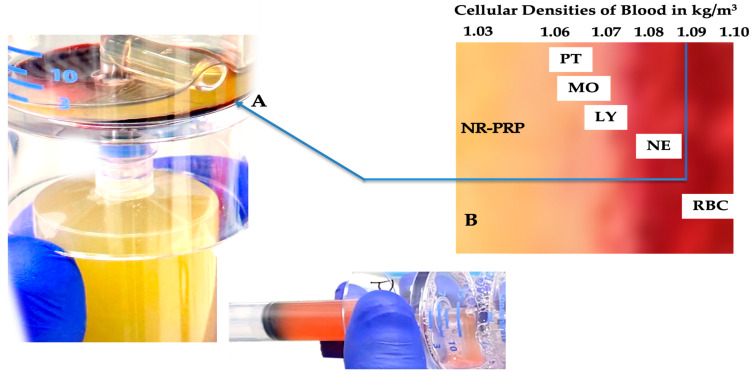
Angiogenesis is the formation of new blood vessel from existing vessels and is a critical first step in tissue repair following chronic disturbances in healing and degenerative tissues. Chronic pathoanatomic tissues are characterized by a high number of inflammatory cells; an overexpression of inflammatory mediators; such as tumor necrosis factor-α (TNF-α) and interleukin-1 (IL-1); the presence of mast cells, T cells, reactive oxygen species, and matrix metalloproteinases; and a decreased angiogenic capacity. Multiple studies have demonstrated that autologous orthobiological cellular preparations (e.g., platelet-rich plasma (PRP)) improve tissue repair and regenerate tissues. There are many PRP devices on the market. Unfortunately, they differ greatly in platelet numbers, cellular composition, and bioformulation. PRP is a platelet concentrate consisting of a high concentration of platelets, with or without certain leukocytes, platelet-derived growth factors (PGFs), cytokines, molecules, and signaling cells. Several PRP products have immunomodulatory capacities that can influence resident cells in a diseased microenvironment, inducing tissue repair or regeneration. Generally, PRP is a blood-derived product, regardless of its platelet number and bioformulation, and the literature indicates both positive and negative patient treatment outcomes. Strangely, the literature does not designate specific PRP preparation qualifications that can potentially contribute to tissue repair. Moreover, the literature scarcely addresses the impact of platelets and leukocytes in PRP on (neo)angiogenesis, other than a general one-size-fits-all statement that "PRP has angiogenic capabilities". Here, we review the cellular composition of all PRP constituents, including leukocytes, and describe the importance of platelet dosing and bioformulation strategies in orthobiological applications to initiate angiogenic pathways that re-establish microvasculature networks, facilitating the supply of oxygen and nutrients to impaired tissues.
Keywords: angiogenesis; bioformulation; biosurgery; leukocytes; orthobiology; platelet dose; platelet-rich fibrin; platelet-rich plasma; tissue repair.
Conflict of interest statement
Peter A. Everts is also the Chief Scientific Officer for EmCyte Corporation.
Figures


References
-
- Everts P.A., Flanagan G., Podesta L. Autologous Orthobiologics. In: Mostoufi S.A., George T.K., Tria A.J. Jr., editors. Clinical Guide to Musculoskeletal Medicine: A Multidisciplinary Approach. Springer International Publishing; Cham, Switzerland: 2022. pp. 651–679.
-
- Magalon J., Brandin T., Francois P., Degioanni C., De Maria L., Grimaud F., Veran J., Dignat-George F., Sabatier F. Technical and Biological Review of Authorized Medical Devices for Platelets-Rich Plasma Preparation in the Field of Regenerative Medicine. Platelets. 2021;32:200–208. doi: 10.1080/09537104.2020.1832653. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
