

Focus on the Most Common Paucisymptomatic Vasculopathic Population, from Diagnosis to Secondary Prevention of Complications
- PMID: 37510100
- PMCID: PMC10377859
- DOI: 10.3390/diagnostics13142356
Focus on the Most Common Paucisymptomatic Vasculopathic Population, from Diagnosis to Secondary Prevention of Complications
Abstract
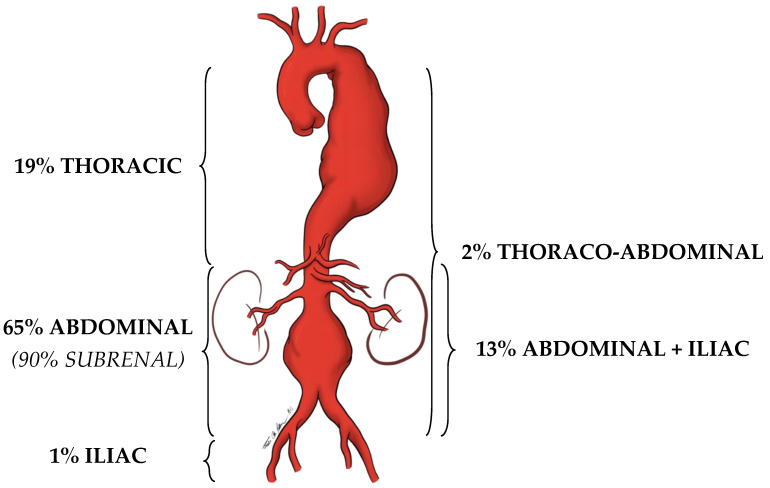
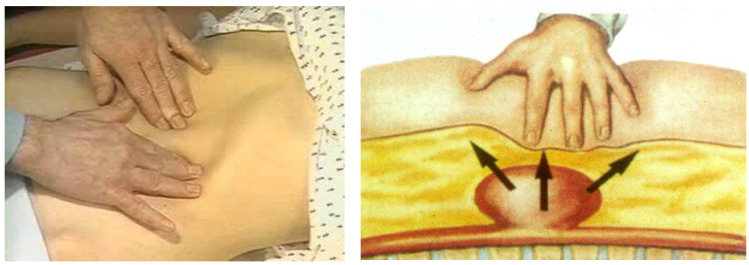
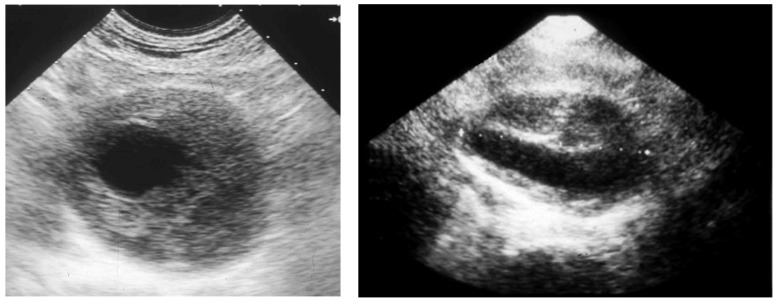
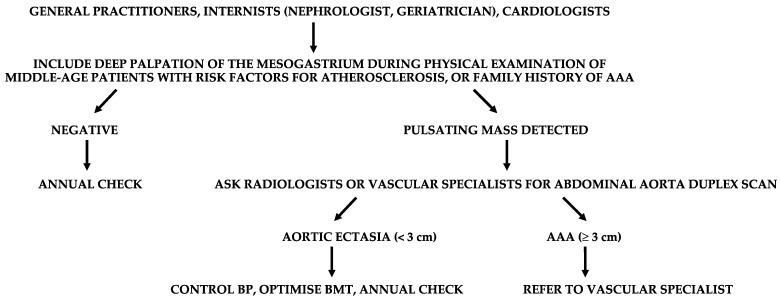
Middle-aged adults can start to be affected by some arterial diseases (ADs), such as abdominal aortic or popliteal artery aneurysms, lower extremity arterial disease, internal carotid, or renal artery or subclavian artery stenosis. These vasculopathies are often asymptomatic or paucisymptomatic before manifesting themselves with dramatic complications. Therefore, early detection of ADs is fundamental to reduce the risk of major adverse cardiovascular and limb events. Furthermore, ADs carry a high correlation with silent coronary artery disease (CAD). This study focuses on the most common ADs, in the attempt to summarize some key points which should selectively drive screening. Since the human and economic possibilities to instrumentally screen wide populations is not evident, deep knowledge of semeiotics and careful anamnesis must play a central role in our daily activity as physicians. The presence of some risk factors for atherosclerosis, or an already known history of CAD, can raise the clinical suspicion of ADs after a careful clinical history and a deep physical examination. The clinical suspicion must then be confirmed by a first-level ultrasound investigation and, if so, adequate treatments can be adopted to prevent dreadful complications.
Keywords: abdominal aortic aneurysm; carotid stenosis; complications; diagnosis; lower extremity arterial disease; popliteal artery aneurysm; renal artery stenosis; secondary prevention; subclavian artery stenosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Johnston K.W., Rutherford R.B., Tilson M.D., Shah D.M., Hollier L., Stanley J.C. Suggested standards for reporting on arterial aneurysms. Subcommittee on Reporting Standards for Arterial Aneurysms, Ad Hoc Committee on Reporting Standards, Society for Vascular Surgery and North American Chapter, International Society for Cardiovascular Surgery. J. Vasc. Surg. 1991;13:452–458. doi: 10.1067/mva.1991.26737. - DOI - PubMed
-
- Chaikof E.L., Dalman R.L., Eskandari M.K., Jackson B.M., Lee W.A., Mansour M.A., Mastracci T.M., Mell M., Murad M.H., Nguyen L.L., et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J. Vasc. Surg. 2018;67:2–77. doi: 10.1016/j.jvs.2017.10.044. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
