

Surgical Anatomy of the Liver-Significance in Ovarian Cancer Surgery
- PMID: 37510115
- PMCID: PMC10378601
- DOI: 10.3390/diagnostics13142371
Surgical Anatomy of the Liver-Significance in Ovarian Cancer Surgery
Abstract
Introduction: Ovarian cancer is the leading cause of death among all gynecological malignancies. Most patients present with an advanced stage of the disease. The routes of spread in ovarian cancer include peritoneal dissemination, direct invasion, and lymphatic or hematogenous spread, with peritoneal and lymphatic spread being the most common among them. The flow direction of the peritoneal fluid makes the right subphrenic space a target site for peritoneal metastases, and the most frequently affected anatomical area in advanced cases is the right upper quadrant. Complete cytoreduction with no macroscopically visible disease is the most important prognostic factor.
Methods: We reviewed published clinical anatomy reports associated with surgery of the liver in cases of advanced ovarian cancer.
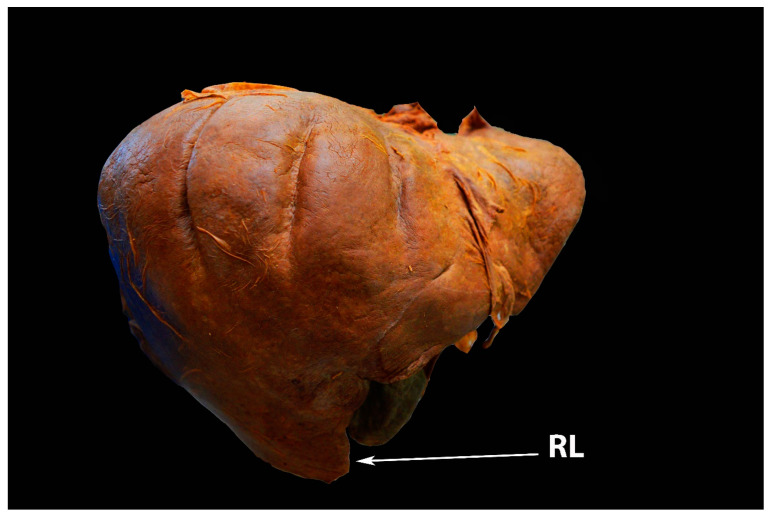
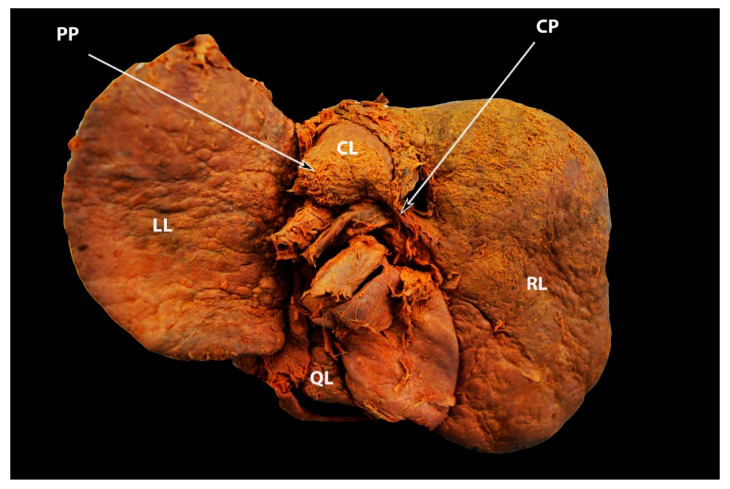
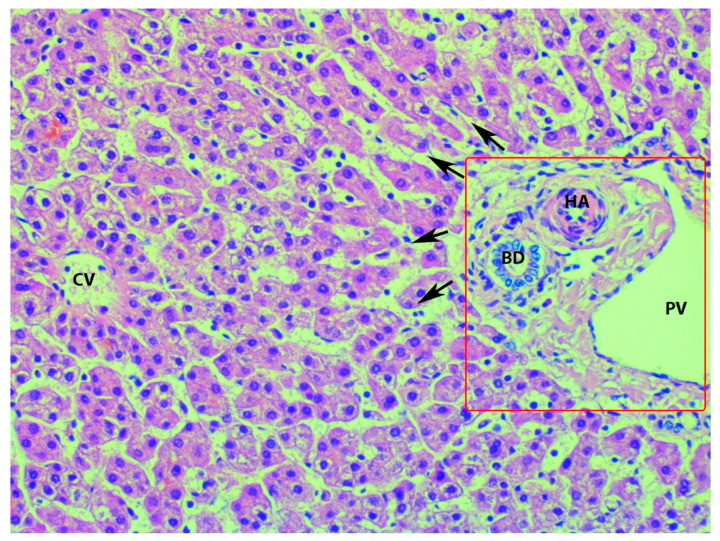
Results: The disease could disseminate anatomical areas, where complex surgery is required-Morrison's pouch, the liver surface, or porta hepatis. The aim of the present article is to emphasize and delineate the gross anatomy of the liver and its surgical application for oncogynecologists. Moreover, the association between the gross and microscopic anatomy of the liver is discussed. Additionally, the vascular supply and variations of the liver are clearly described.
Conclusions: Oncogynecologists performing liver mobilization, diaphragmatic stripping, and porta hepatis dissection must have a thorough knowledge of liver anatomy, including morphology, variations, functional status, potential diagnostic imaging mistakes, and anatomical limits of dissection.
Keywords: anatomical variations; hepatic veins; liver anatomy; liver ligaments; liver morphology; ovarian cancer surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

























References
-
- Taskiran C., Vatansever D., Giray B., Eraslan A., Tanju S., Arvas M., Balik E. Upper abdominal debulking surgery for ovarian cancer total colectomy, total peritonectomy, and extended upper abdominal debulking surgery. Int. J. Gynecol. Cancer. 2020;30:1648–1649. doi: 10.1136/ijgc-2020-001531. - DOI - PubMed
-
- Aletti G.D., Dowdy S.C., Gostout B.S., Jones M.B., Stanhope C.R., Wilson T.O., Podratz K.C., Cliby W.A. Aggressive surgical effort and improved survival in advanced-stage ovarian cancer. Obs. Gynecol. 2006;107:77–85. doi: 10.1097/01.AOG.0000192407.04428.bb. - DOI - PubMed
-
- Bristow R.E., Karlan B.Y., Chi D.S. Surgery for Ovarian Cancer. 3rd ed. Taylor & Francis Group, LLC.; Abingdon, UK: 2016.
Publication types
LinkOut - more resources
Full Text Sources
