

Detecting Diabetic Ketoacidosis with Infection: Combating a Life-Threatening Emergency with Practical Diagnostic Tools
- PMID: 37510185
- PMCID: PMC10378387
- DOI: 10.3390/diagnostics13142441
Detecting Diabetic Ketoacidosis with Infection: Combating a Life-Threatening Emergency with Practical Diagnostic Tools
Abstract
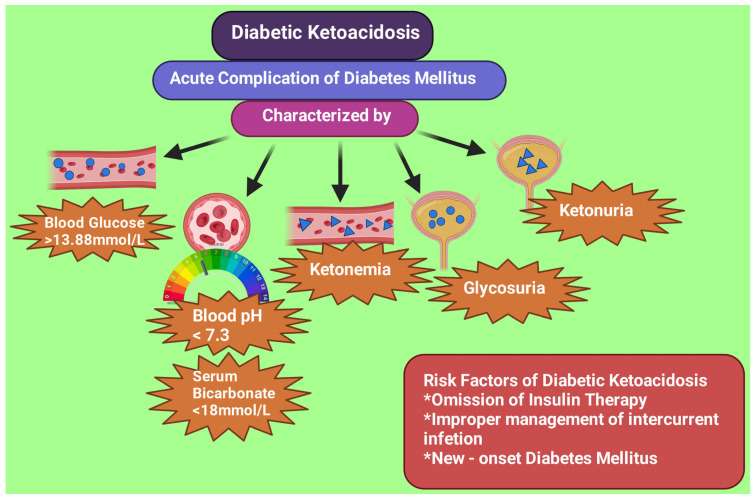
Background: Diabetic ketoacidosis (DKA) is a life-threatening acute complication of diabetes mellitus and can lead to patient demise if not immediately treated. From the recent literature, the diabetic ketoacidosis mortality rate, depending on age, is 2-5%. Insulin discontinuation and infection remain the two most common triggers for diabetic ketoacidosis. About 50% of cases of ketoacidosis result from bacterial infections like urinary tract infections and pneumonia. It is also important to diagnose the presence of infection in diabetic ketoacidosis patients to prevent the excessive use of antibiotics, which may lead to antibiotic resistance. Although performing bacterial culture is confirmatory for the presence or absence of bacterial infection, the time required to obtain the result is long. At the same time, emergency treatment needs to be started as early as possible.
Methods: This narrative review examines various septic markers to identify the appropriate tools for diagnosis and to distinguish between diabetic ketoacidosis with and without infection. Electronic databases were searched using the Google engine with the keywords "Diabetes Mellitus", "Diabetic Ketoacidosis", "Infection with Diabetic Ketoacidosis", "biomarkers for infection in Diabetic Ketoacidosis", "Procalcitonin", "Inflammatory cytokines in DKA", "Lactic acidosis in DKA", and "White blood cell in infection in DKA".
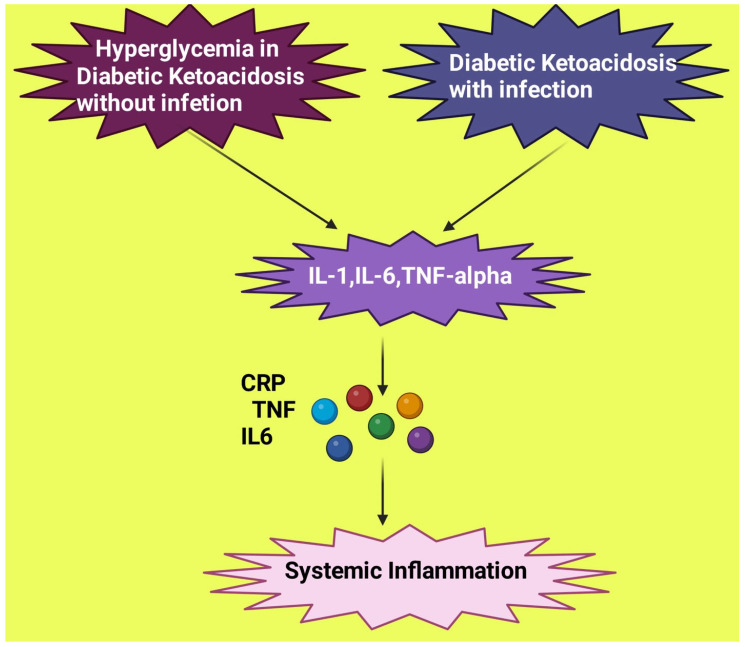
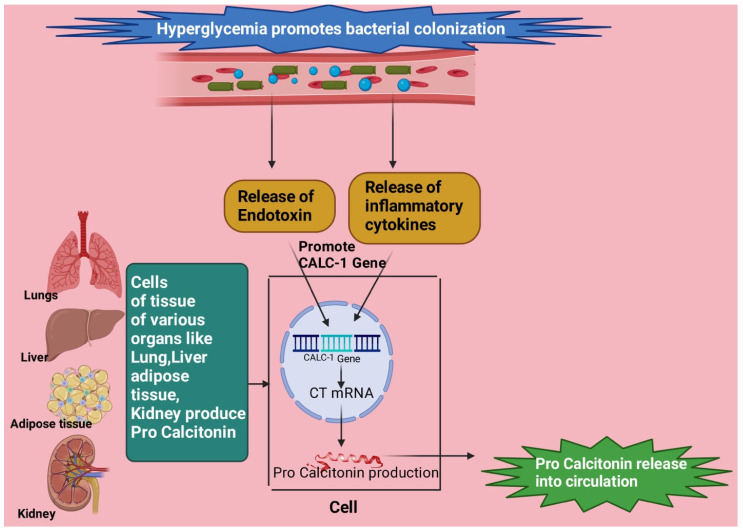
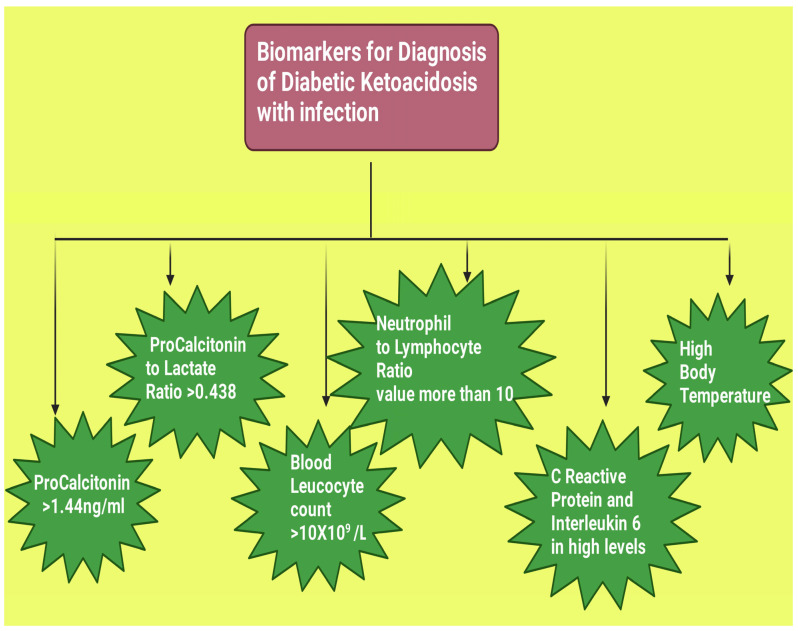
Results: This narrative review article presents the options for diagnosis and also aims to create awareness regarding the gravity of diabetic ketoacidosis with infection and emphasizes the importance of early diagnosis for appropriate management. Diabetes mellitus is a clinical condition that may lead to several acute and chronic complications. Acute diabetic ketoacidosis is a life-threatening condition in which an excess production of ketone bodies results in acidosis and hypovolemia. Infection is one of the most common triggers of diabetic ketoacidosis. When bacterial infection is present along with diabetic ketoacidosis, the mortality rate is even higher than for patients with diabetic ketoacidosis without infection. The symptoms and biomarkers of diabetic ketoacidosis are similar to that of infection, like fever, C reactive protein, and white blood cell count, since both create an environment of systemic inflammation. It is also essential to distinguish between the presence and absence of bacterial infection to ensure the appropriate use of antibiotics and prevent antimicrobial resistance. A bacterial culture report is confirmatory for the existence of bacterial infection, but this may take up to 24 h. Diagnosis needs to be performed approximately in the emergency room upon admission since there is a need for immediate management. Therefore, researching the possible diagnostic tools for the presence of infection in diabetic ketoacidosis patients is of great importance. Several of such biomarkers have been discussed in this research work.
Keywords: bacterial infection; biomarkers; diabetic ketoacidosis; early diagnosis; emergency; inflammation; sepsis.
Conflict of interest statement
The authors declare no conflict of interest. The author declares that they do not have any financial involvement or affiliations with any organization, association, or entity directly or indirectly involved with the subject matter or materials presented in this article. This includes honoraria, expert testimony, employment, the ownership of stocks or options, patents or grants received or pending, or royalties.
Figures
References
-
- Savage M.W., Dhatariya K.K., Kilvert A., Rayman G., Rees J.A., Courtney C.H., Hilton L., Dyer P.H., Hamersley M.S., Joint British Diabetes Societies Joint British Diabetes Societies guideline for the management of diabetic ketoacidosis. Diabet. Med. 2011;28:508–515. doi: 10.1111/j.1464-5491.2011.03246.x. - DOI - PubMed
-
- Cheng Y.C., Huang C.H., Lin W.R., Lu P.L., Chang K., Tsai J.J., Bojang K.S., Lin C.Y., Chen Y.H. Clinical outcomes of septic patients with diabetic ketoacidosis between 2004 and 2013 in a tertiary hospital in Taiwan. J. Microbiol. Immunol. Infect. 2016;49:663–671. doi: 10.1016/j.jmii.2014.08.018. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
