

Patient Perspectives on Digital Interventions to Manage Heart Failure Medications: The VITAL-HF Pilot
- PMID: 37510791
- PMCID: PMC10380884
- DOI: 10.3390/jcm12144676
Patient Perspectives on Digital Interventions to Manage Heart Failure Medications: The VITAL-HF Pilot
Abstract
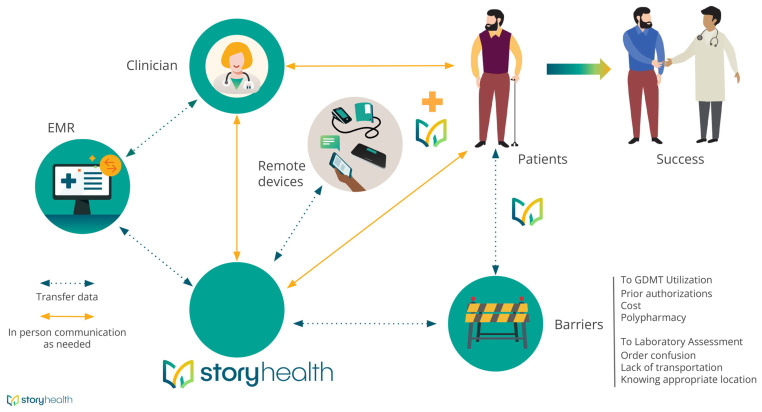
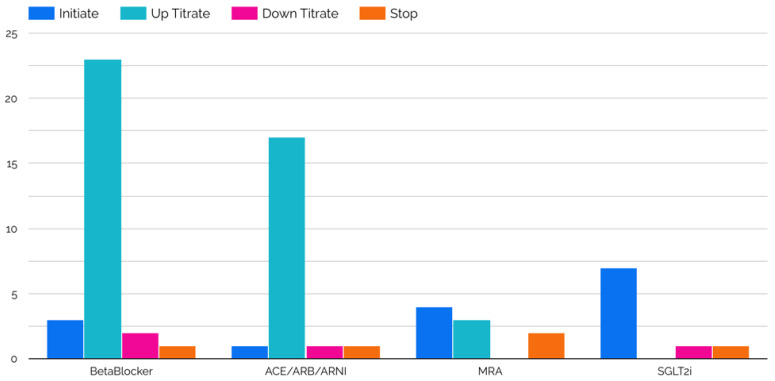
Use of guideline-directed medical therapy (GDMT) for treatment of heart failure with reduced ejection fraction (HFrEF) remains unacceptably low. The purpose of this study was to determine whether a digital health tool can augment GDMT for patients with HFrEF. Participants ≥ 18 years old with symptomatic HFrEF (left ventricular ejection fraction ≤ 40%) and with access to a mobile phone with internet were included. Participants were given a blood pressure cuff, instructed in its use, and given regular symptom surveys via cell-phone web-link. Data were transmitted to the Story Health web-based platform, and automated alerts were triggered based on pre-specified vital sign and laboratory data. Health coaches assisted patients with medication education, pharmacy access, and lab access through text messages and phone calls. GDMT titration plans were individually created in the digital platform by local clinicians based on entry vitals and labs. Twelve participants enrolled and completed the study. The median age and LVEF were 52.5 years (IQR, 46.5-63.5) and 25% (IQR, 22.5-35.5), respectively. There were 10 GDMT initiations, 52 up-titrations, and 13 down-titrations. Five participants engaged in focus-group interviews following study completion to understand first-hand perspectives regarding the use of digital tools to manage GDMT. Participants expressed comfort knowing that there were clinicians regularly reviewing their data. This alleviated concerns of uncertainty in daily living, led to an increased feeling of security, and empowered patients to understand decision-making regarding GDMT. Frequent medication changes, and the associated financial impact, were common concerns. Remote titration of GDMT for HFrEF is feasible and appears to be a patient-centered approach to care.
Keywords: digital health; guideline-directed medical therapy; remote monitoring; virtual health.
Conflict of interest statement
Dr DeVore reports research funding through his institution from the American Heart Association, Biofourmis, Bodyport, Cytokinetics, American Regent, Inc., the NHLBI, Novartis, and Story Health. He also provides consulting services for and/or receives honoraria from Abiomed, AstraZeneca, Cardionomic, InnaMed, LivaNova, Natera, Novartis, Procyrion, Story Health, Vifor, and Zoll. He has also received non-financial support from Abbott for educational and research activities.
Figures


References
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., Anderson C.A.M., Arora P., Avery C.L., Baker-Smith C.M., Beaton A.Z., Boehme A.K., Buxton A.E., et al. Heart Disease and Stroke Statistics—2023 Update: A Report From the American Heart Association. Circulation. 2023;147:e93–e621. - PubMed
-
- Heidenreich P.A., Bozkurt B., Aguilar D., Allen L.A., Byun J.J., Colvin M.M., Deswal A., Drazner M.H., Dunlay S.M., Evers L.R., et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e895–e1032. - PubMed
-
- McDonagh T.A., Metra M., Adamo M., Gardner R.S., Baumbach A., Böhm M., Burri H., Butler J., Čelutkienė J., Chioncel O., et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021;42:3599–3726. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
