

Defining the Role of Anaortic Coronary Artery Bypass Grafting
- PMID: 37510812
- PMCID: PMC10380961
- DOI: 10.3390/jcm12144697
Defining the Role of Anaortic Coronary Artery Bypass Grafting
Abstract
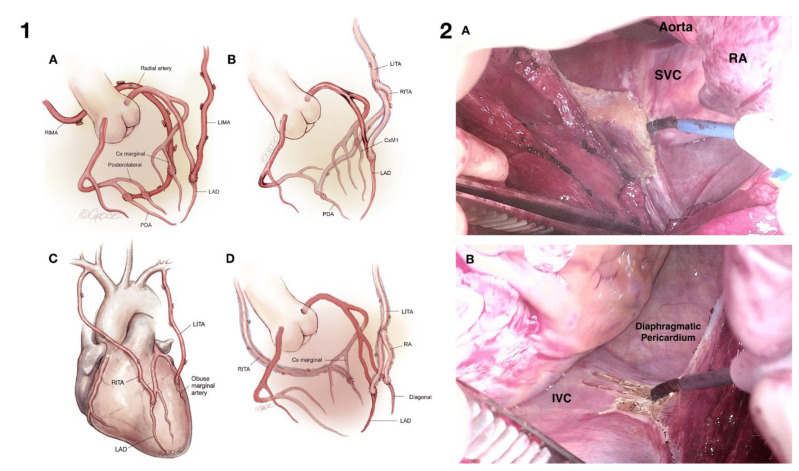
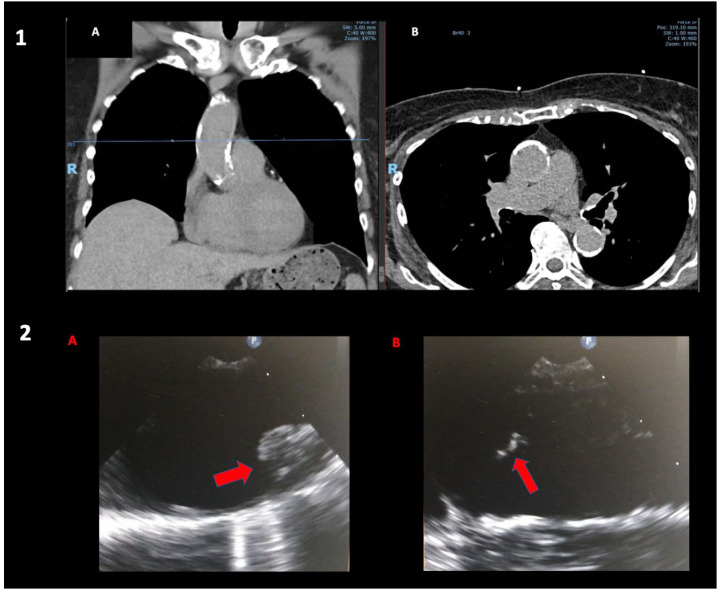
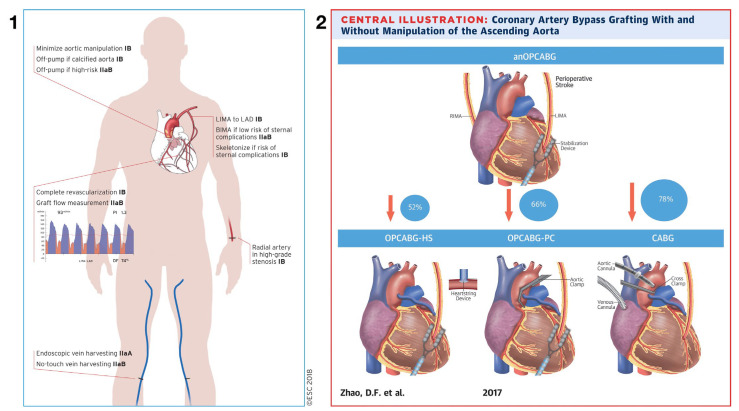
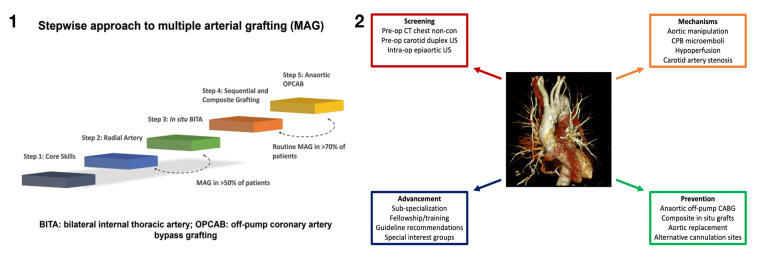
As the population ages and co-morbidities become more prevalent, the complexity of patients presenting for coronary artery bypass surgery is increasing. Cardiopulmonary bypass and aortic cross-clamping in these patients carry increased risk and, indeed, in some patients, with ascending aortic disease, the risks are prohibitive. Total-arterial anaortic coronary artery surgery is a technique that provides complete surgical coronary artery revascularization without cardiopulmonary bypass and without manipulating the ascending aorta. The technique essentially eliminates the risk of cerebral embolization of aortic atheroma and aortic injury. Anaortic techniques are an essential skillset for coronary artery surgery centers treating higher-risk patients.
Keywords: anaortic; coronary surgery; off-pump; stroke.
Conflict of interest statement
The authors declare no conflictS of interest.
Figures
Similar articles
-
Toward stroke-free coronary surgery: The role of the anaortic off-pump bypass technique.J Card Surg. 2021 Apr;36(4):1499-1510. doi: 10.1111/jocs.15372. Epub 2021 Jan 27. J Card Surg. 2021. PMID: 33502822 Review.
-
Anaortic techniques reduce neurological morbidity after off-pump coronary artery bypass surgery.Heart Lung Circ. 2008 Aug;17(4):299-304. doi: 10.1016/j.hlc.2007.11.138. Epub 2008 Feb 21. Heart Lung Circ. 2008. PMID: 18294911
-
Concomitant anaortic OPCAB and transfemoral TAVR for high-risk patients: A case series.J Card Surg. 2022 Nov;37(11):3935-3942. doi: 10.1111/jocs.16838. Epub 2022 Sep 13. J Card Surg. 2022. PMID: 36098378
-
Neurologic complications after off-pump coronary artery bypass grafting with and without aortic manipulation: meta-analysis of 11,398 cases from 8 studies.J Thorac Cardiovasc Surg. 2011 Aug;142(2):e11-7. doi: 10.1016/j.jtcvs.2010.11.034. Epub 2011 Feb 1. J Thorac Cardiovasc Surg. 2011. PMID: 21281950
-
The Anaortic Technique with Bilateral Internal Thoracic Artery Grafting - Filling the Gap in Coronary Artery Bypass Surgery.Braz J Cardiovasc Surg. 2021 Jun 1;36(3):397-405. doi: 10.21470/1678-9741-2020-0451. Braz J Cardiovasc Surg. 2021. PMID: 34387975 Free PMC article. Review.
Cited by
-
The frail patient undergoing cardiac surgery: lessons learned and future perspectives.Front Cardiovasc Med. 2023 Dec 6;10:1295108. doi: 10.3389/fcvm.2023.1295108. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 38124896 Free PMC article. Review.
References
-
- Zhao D.F., Edelman J.J., Seco M., Bannon P.G., Wilson M.K., Byrom M.J., Thourani V., Lamy A., Taggart D.P., Puskas J.D., et al. Coronary Artery Bypass Grafting with and Without Manipulation of the Ascending Aorta: A Network Meta-Analysis. J. Am. Coll. Cardiol. 2017;69:924–936. doi: 10.1016/j.jacc.2016.11.071. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
