

The Role of Multimodality Imaging in Pediatric Cardiomyopathies
- PMID: 37510983
- PMCID: PMC10381492
- DOI: 10.3390/jcm12144866
The Role of Multimodality Imaging in Pediatric Cardiomyopathies
Abstract
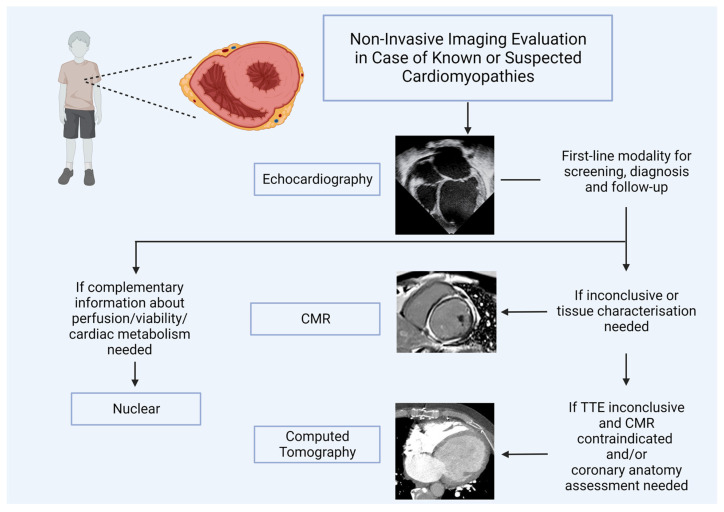
Cardiomyopathies are a heterogeneous group of myocardial diseases representing the first cause of heart transplantation in children. Diagnosing and classifying the different phenotypes can be challenging, particularly in this age group, where cardiomyopathies are often overlooked until the onset of severe symptoms. Cardiovascular imaging is crucial in the diagnostic pathway, from screening to classification and follow-up assessment. Several imaging modalities have been proven to be helpful in this field, with echocardiography undoubtedly representing the first imaging approach due to its low cost, lack of radiation, and wide availability. However, particularly in this clinical context, echocardiography may not be able to differentiate from cardiomyopathies with similar phenotypes and is often complemented with cardiovascular magnetic resonance. The latter allows a radiation-free differentiation between different phenotypes with unique myocardial tissue characterization, thus identifying the presence and extent of myocardial fibrosis. Nuclear imaging and computed tomography have a complementary role, although they are less used in daily clinical practice due to the concern related to the use of radiation in pediatric patients. However, these modalities may have some advantages in evaluating children with cardiomyopathies. This paper aims to review the strengths and limitations of each imaging modality in evaluating pediatric patients with suspected or known cardiomyopathies.
Keywords: cardiovascular multimodality imaging; pediatric cardiology; pediatric cardiomyopathy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Lipshultz S.E., Law Y.M., Asante-Korang A., Austin E.D., Dipchand A.I., Everitt M.D., Hsu D.T., Lin K.Y., Price J.F., Wilkinson J.D., et al. Cardiomyopathy in Children: Classification and Diagnosis: A Scientific Statement from the American Heart Association. Circulation. 2019;140:e9–e68. doi: 10.1161/CIR.0000000000000682. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
