

Randomized Clinical Trials and Observational Tribulations: Providing Clinical Evidence for Personalized Surgical Pain Management Care Models
- PMID: 37511657
- PMCID: PMC10381640
- DOI: 10.3390/jpm13071044
Randomized Clinical Trials and Observational Tribulations: Providing Clinical Evidence for Personalized Surgical Pain Management Care Models
Abstract
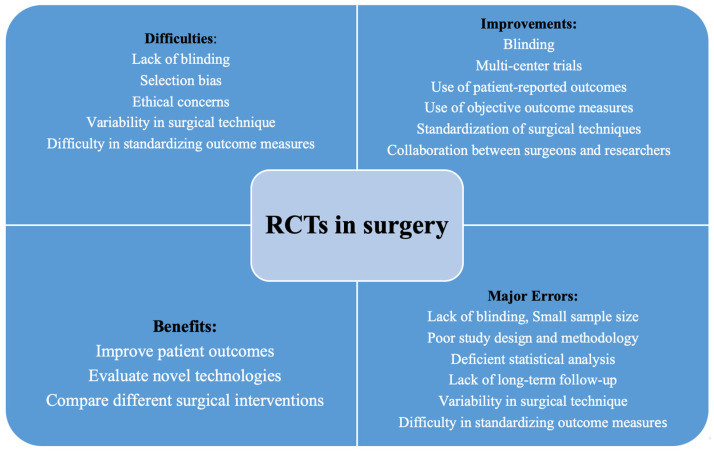
Proving clinical superiority of personalized care models in interventional and surgical pain management is challenging. The apparent difficulties may arise from the inability to standardize complex surgical procedures that often involve multiple steps. Ensuring the surgery is performed the same way every time is nearly impossible. Confounding factors, such as the variability of the patient population and selection bias regarding comorbidities and anatomical variations are also difficult to control for. Small sample sizes in study groups comparing iterations of a surgical protocol may amplify bias. It is essentially impossible to conceal the surgical treatment from the surgeon and the operating team. Restrictive inclusion and exclusion criteria may distort the study population to no longer reflect patients seen in daily practice. Hindsight bias is introduced by the inability to effectively blind patient group allocation, which affects clinical result interpretation, particularly if the outcome is already known to the investigators when the outcome analysis is performed (often a long time after the intervention). Randomization is equally problematic, as many patients want to avoid being randomly assigned to a study group, particularly if they perceive their surgeon to be unsure of which treatment will likely render the best clinical outcome for them. Ethical concerns may also exist if the study involves additional and unnecessary risks. Lastly, surgical trials are costly, especially if the tested interventions are complex and require long-term follow-up to assess their benefit. Traditional clinical testing of personalized surgical pain management treatments may be more challenging because individualized solutions tailored to each patient's pain generator can vary extensively. However, high-grade evidence is needed to prompt a protocol change and break with traditional image-based criteria for treatment. In this article, the authors review issues in surgical trials and offer practical solutions.
Keywords: clinical evidence; pain generators; personalized care models; surgical clinical trials.
Conflict of interest statement
There was no formal funding by private, governmental, or commercial funders. The participating spine centers (Center For Advanced Spine Care of Southern Arizona—Tucson, Arizona; Desert Institute of Spine Care—Phoenix, Arizona; Department of Orthopaedics, Fundación Universitaria Sanitas—Bogotá, D.C., Colombia; Department of Neurosurgery and Orthopaedics at Hospital Universitário Gaffre e Guinle, Universidade Federal do Estado do Rio de Janeiro—Rio de Janeiro, Brazil; Department of Orthopaedic Surgery, The First Affiliated Hospital of Soochow University; The American–British Cowdray Medical Center; Good Doctor Teun Teun Spine Hospital; Endoscopic Spine Clinic, Santiago, Chile; Department of Neurosurgery, Nanoori Hospital Gangnam Hospital; West China Hospital of Sichuan University supported, with their internal resources, the design and conduction of this study. They aided in the collection, analysis, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results. The authors declare no conflict of interest to the work presented herein, including no personal circumstances or interests that may be perceived as inappropriately influencing the representation or interpretation of the research data or professional information.
Figures
References
-
- Joeris A., Knoll C., Kalampoki V., Blumenthal A., Gaskell G. Patient-reported outcome measurements in clinical routine of trauma, spine and craniomaxillofacial surgeons: Between expectations and reality: A survey among 1212 surgeons. BMJ Open. 2018;8:e020629. doi: 10.1136/bmjopen-2017-020629. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
