

Dual Antiplatelet Therapy: A Concise Review for Clinicians
- PMID: 37511955
- PMCID: PMC10381391
- DOI: 10.3390/life13071580
Dual Antiplatelet Therapy: A Concise Review for Clinicians
Abstract
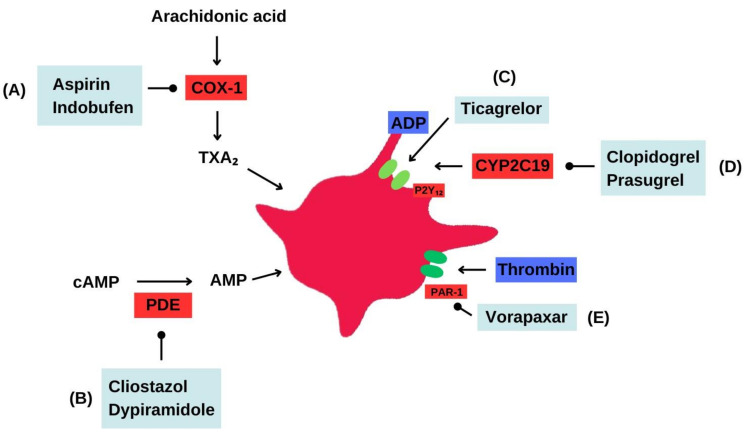
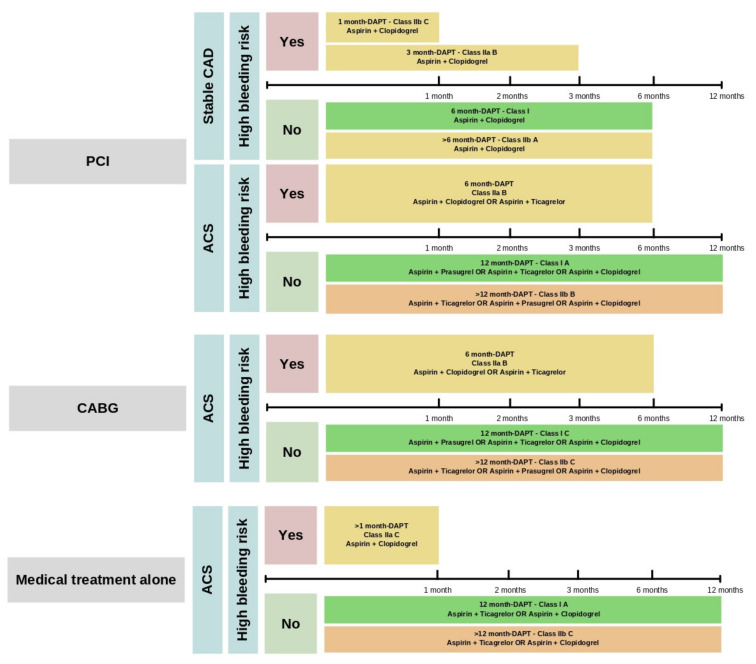
Dual antiplatelet therapy (DAPT) combines two antiplatelet agents to decrease the risk of thrombotic complications associated with atherosclerotic cardiovascular diseases. Emerging data about the duration of DAPT is being published continuously. New approaches are trying to balance the time, benefits, and risks for patients taking DAPT for established cardiovascular diseases. Short-term dual DAPT of 3-6 months, or even 1 month in high-bleeding risk patients, is equivalent in terms of efficacy and effectiveness compared to long-term DAPT for patients who experienced percutaneous coronary intervention in an acute coronary syndrome setting. Prolonged DAPT beyond 12 months reduces stent thrombosis, major adverse cardiovascular events, and myocardial infarction rates but increases bleeding risk. Extended DAPT does not significantly benefit stable coronary artery disease patients in reducing stroke, myocardial infarction, or cardiovascular death. Ticagrelor and aspirin reduce cardiovascular events in stable coronary artery disease with diabetes but carry a higher bleeding risk. Antiplatelet therapy duration in atrial fibrillation patients after percutaneous coronary intervention depends on individual characteristics and bleeding risk. Antiplatelet therapy is crucial for post-coronary artery bypass graft and transcatheter aortic valve implantation; Aspirin (ASA) monotherapy is preferred. Antiplatelet therapy duration in peripheral artery disease depends on the scenario. Adding vorapaxar and cilostazol may benefit secondary prevention and claudication, respectively. Carotid artery disease patients with transient ischemic attack or stroke benefit from antiplatelet therapy and combining ASA and clopidogrel is more effective than ASA alone. The optimal duration of DAPT after carotid artery stenting is uncertain. Resistance to ASA and clopidogrel poses an incremental risk of deleterious cardiovascular events and stroke. The selection and duration of antiplatelet therapy in patients with cardiovascular disease requires careful consideration of both efficacy and safety outcomes. The use of combination therapies may provide added benefits but should be weighed against the risk of bleeding. Further research and clinical trials are needed to optimize antiplatelet treatment in different patient populations and clinical scenarios.
Keywords: DAPT; dual antiplatelet therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Levine G.N., Bates E.R., Bittl J.A., Brindis R.G., Fihn S.D., Fleisher L.A., Granger C.B., Lange R.A., Mack M.J., Mauri L., et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease. J. Am. Coll. Cardiol. 2016;68:1082–1115. doi: 10.1016/j.jacc.2016.03.513. - DOI - PubMed
-
- Valgimigli M., Bueno H., Byrne R.A., Collet J.P., Costa F., Jeppsson A., Jüni P., Kastrati A., Kolh P., Mauri L., et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS) Eur. Heart J. 2018;39:213–260. - PubMed
-
- Urban P., Mehran R., Colleran R., Angiolillo D.J., Byrne R.A., Capodanno D., Cuisset T., Cutlip D., Eerdmans P., Eikelboom J., et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention: A consensus document from the Academic Research Consortium for High Bleeding Risk. Eur. Heart J. 2019;40:2632–2653. doi: 10.1093/eurheartj/ehz372. - DOI - PMC - PubMed
-
- Biasco L., Montrasio G., Moccetti M., Pedrazzini G. Current trends in dual antiplatelet therapy: A 2017 update. Cardiovasc. Med. 2017;20:169–175.
Publication types
LinkOut - more resources
Full Text Sources
