

Transcatheter Arterial Embolization (TAE) of Cancer-Related Bleeding
- PMID: 37512135
- PMCID: PMC10383256
- DOI: 10.3390/medicina59071323
Transcatheter Arterial Embolization (TAE) of Cancer-Related Bleeding
Abstract
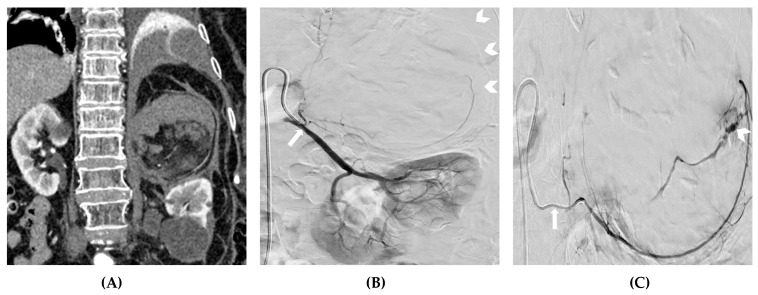
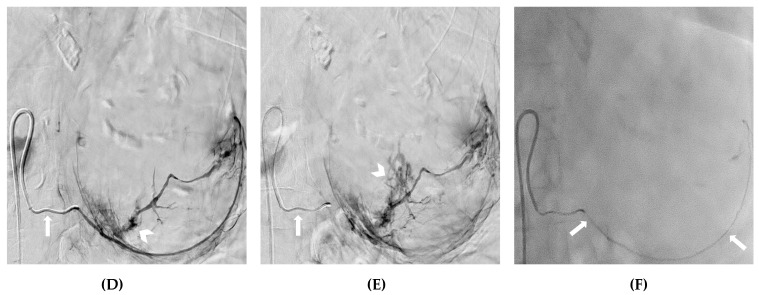
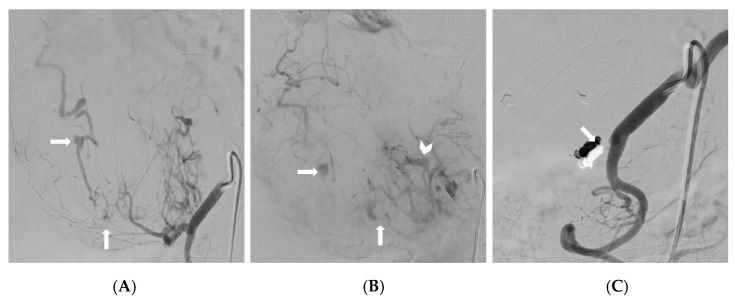
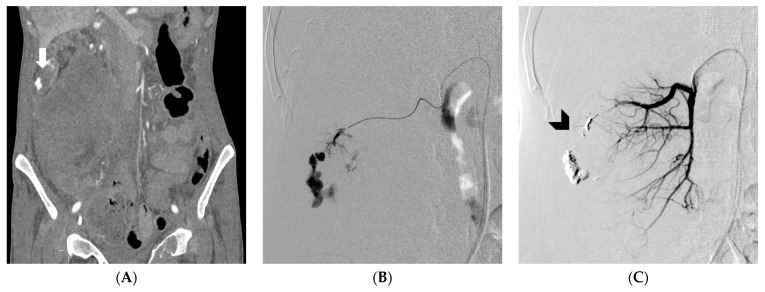
Background and Objectives: Roughly 10% of cancer patients experience an episode of bleeding. The bleeding severity can range from occasional trivial bleeds to major bleeding. The treatment for the bleeding may vary, depending on the clinical condition and anatomical site, and may include various strategies, among which TAE is a cornerstone of major bleeding management. However, the existing literature on tumor hemorrhages is inconsistent. The objective of this multicenter retrospective cohort study was to evaluate the effectiveness and safety of arterial embolization in the treatment of tumor hemorrhages in patients with solid cancers. Materials and Methods: The data for patients with solid cancers undergoing TAE for the management of tumor hemorrhages from January 2020 to May 2023 were gathered. Results: A total of 92 patients with cancer-related bleeding were treated between January 2020 and May 2023. No bleeding was detected by X-ray angiography (XA) in 12 (13%) cases; therefore, a blind embolization was performed. The most common bleeding site was the liver (21.7%). A total of 66 tumor hemorrhages were spontaneous. The most commonly used embolic agent was polyvinyl alcohol (PVA) particles (30.4%). Technical success was achieved in 82 (89.1%) cases, with an 84.8% clinical success rate related to 14 cases of rebleeding. Proximal embolization was performed for 19 (20.7%) patients. Complications were recorded for 10 (10.9%) patients. The 30-day bleeding-related mortality was 15.2%. The technical success, clinical success, proximal embolization rate, and 30-day rebleeding were worse in the subset of patients undergoing TAE with coils. Conclusions: Transcatheter arterial embolization (TAE) represents a viable and potentially life-saving therapeutic approach in the management of tumor hemorrhages, demonstrating a notable effectiveness and safety. The TAE of bleeding tumors using coils resulted in a higher rate of non-superselective proximal embolization, with a trend toward lower clinical success rates and higher rebleeding episodes.
Keywords: TAE; bleeding; cancer; embolic agents; embolization; endovascular; hemorrhage; tumor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Schulman S., Kearon C., Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005;3:692–694. doi: 10.1111/j.1538-7836.2005.01204.x. - DOI - PubMed
-
- European Medicines Agency Clinical Investigation of Medicinal Products for the Prophylaxis of Venous Thromboembolic Risk in Non-Surgical Patients—Scientific Guideline. [(accessed on 20 May 2023)]. Available online: https://www.ema.europa.eu/en/clinical-investigation-medicinal-products-p....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
