

Pulmonary Co-Infections Detected Premortem Underestimate Postmortem Findings in a COVID-19 Autopsy Case Series
- PMID: 37513779
- PMCID: PMC10383307
- DOI: 10.3390/pathogens12070932
Pulmonary Co-Infections Detected Premortem Underestimate Postmortem Findings in a COVID-19 Autopsy Case Series
Abstract
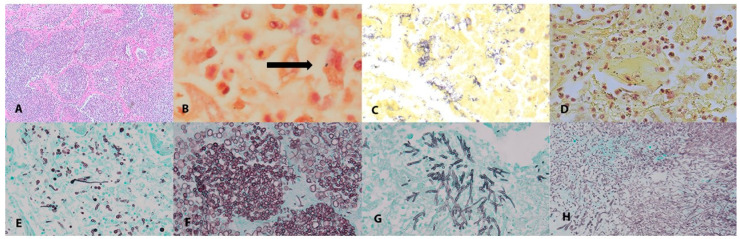
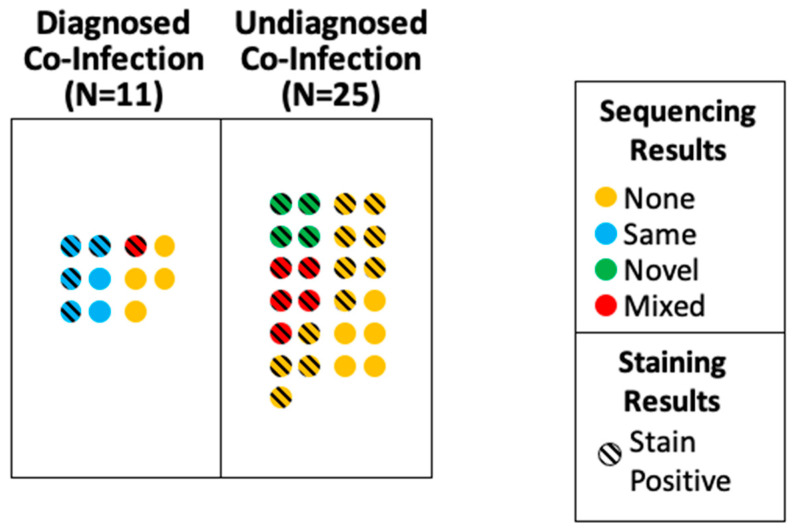
Bacterial and fungal co-infections are reported complications of coronavirus disease 2019 (COVID-19) in critically ill patients but may go unrecognized premortem due to diagnostic limitations. We compared the premortem with the postmortem detection of pulmonary co-infections in 55 fatal COVID-19 cases from March 2020 to March 2021. The concordance in the premortem versus the postmortem diagnoses and the pathogen identification were evaluated. Premortem pulmonary co-infections were extracted from medical charts while applying standard diagnostic definitions. Postmortem co-infection was defined by compatible lung histopathology with or without the detection of an organism in tissue by bacterial or fungal staining, or polymerase chain reaction (PCR) with broad-range bacterial and fungal primers. Pulmonary co-infection was detected premortem in significantly fewer cases (15/55, 27%) than were detected postmortem (36/55, 65%; p < 0.0001). Among cases in which co-infection was detected postmortem by histopathology, an organism was identified in 27/36 (75%) of cases. Pseudomonas, Enterobacterales, and Staphylococcus aureus were the most frequently identified bacteria both premortem and postmortem. Invasive pulmonary fungal infection was detected in five cases postmortem, but in no cases premortem. According to the univariate analyses, the patients with undiagnosed pulmonary co-infection had significantly shorter hospital (p = 0.0012) and intensive care unit (p = 0.0006) stays and significantly fewer extra-pulmonary infections (p = 0.0021). Bacterial and fungal pulmonary co-infection are under-recognized complications in critically ill patients with COVID-19.
Keywords: COVID-19; autopsy; co-infection; invasive fungal infections; nosocomial infections; pneumonia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Shieh W.J., Blau D.M., Denison A.M., Deleon-Carnes M., Adem P., Bhatnagar J., Sumner J., Liu L., Patel M., Batten B., et al. 2009 pandemic influenza A (H1N1): Pathology and pathogenesis of 100 fatal cases in the United States. Am. J. Pathol. 2010;177:166–175. doi: 10.2353/ajpath.2010.100115. - DOI - PMC - PubMed
-
- Rouze A., Martin-Loeches I., Povoa P., Makris D., Artigas A., Bouchereau M., Lambiotte F., Metzelard M., Cuchet P., Boulle Geronimi C., et al. Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: A European multicenter cohort study. Intensive Care Med. 2021;47:188–198. doi: 10.1007/s00134-020-06323-9. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
