

The effectiveness of the puncture channel plugging for reduction of complications after CT-guided percutaneous transthoracic needle biopsy
- PMID: 37516777
- PMCID: PMC10387056
- DOI: 10.1038/s41598-023-38915-y
The effectiveness of the puncture channel plugging for reduction of complications after CT-guided percutaneous transthoracic needle biopsy
Abstract
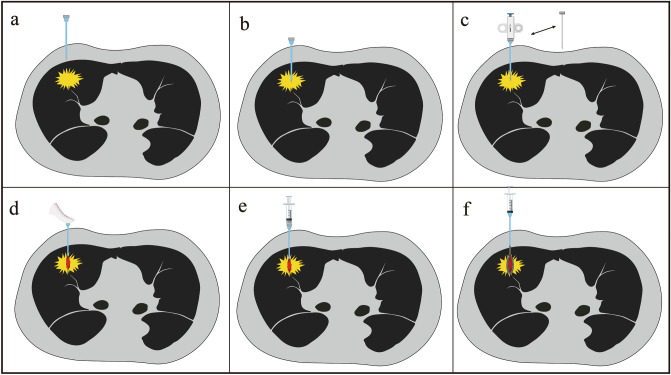
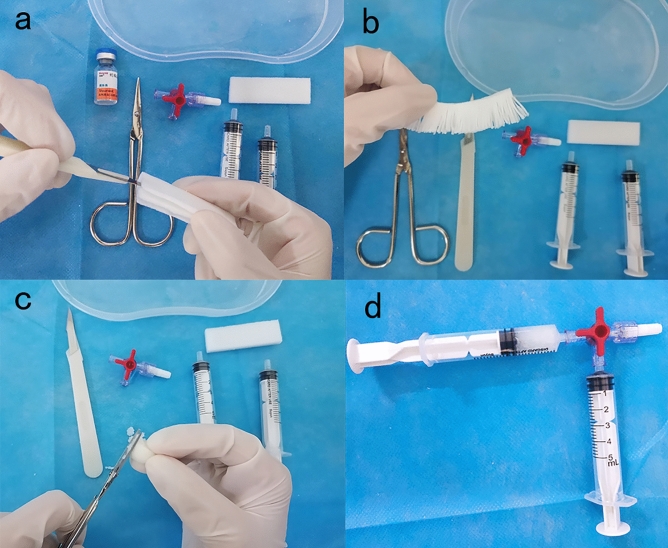
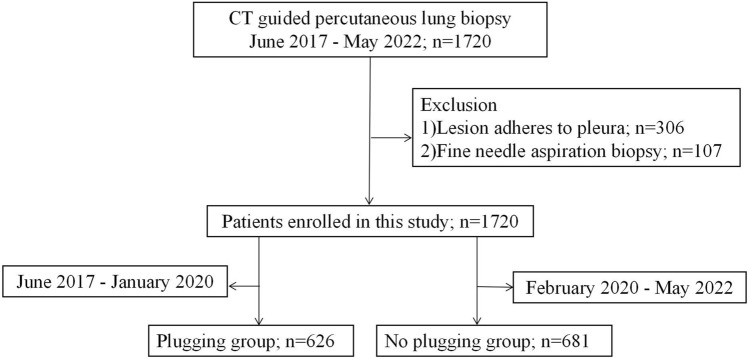
The effect of plugging the puncture channel with a mixture of hemocoagulase injection on the complications of CT-guided percutaneous transthoracic need biopsy (PTNB) was discussed. The medical records of PTNB were retrospectively studied from June 2017 to May 2022. In the study, the puncture channel of 626 patients were blocked, while remain 681 patients' were not. The Mantel Haenszel method performed layered analysis and evaluated the correlation of adjusted confounding factors. The Odds Ratio and its 95% confidence interval were calculated using the Woof method. The incidence of high-level pulmonary hemorrhage was significantly reduced in patients with lesions ≤ 2 cm and different needle lengths. Patients with different pleural-needle tip angle and perineedle emphysema were blocked, and the incidence of pneumothorax and thoracic implants was significantly reduced. Through puncture channel plugging, the incidence of pulmonary hemorrhage, pneumothorax and thoracic catheterization of PTNB under CT guidance was reduced.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Yoon SH, Lee SM, Park CH, et al. 2020 clinical practice guideline for percutaneous transthoracic needle biopsy of pulmonary lesions: A consensus statement and recommendations of the Korean society of thoracic radiology. Korean J. Radiol. 2021;22(2):263–280. doi: 10.3348/kjr.2020.0137. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
