

Incidence and outcomes of acute kidney injury including hepatorenal syndrome in hospitalized patients with cirrhosis in the US
- PMID: 37517455
- PMCID: PMC10807505
- DOI: 10.1016/j.jhep.2023.07.010
Incidence and outcomes of acute kidney injury including hepatorenal syndrome in hospitalized patients with cirrhosis in the US
Abstract
Background & aims: Acute kidney injury (AKI) in cirrhosis is common and associated with high morbidity, but the incidence rates of different etiologies of AKI are not well described in the US. We compared incidence rates, practice patterns, and outcomes across etiologies of AKI in cirrhosis.
Methods: We performed a retrospective cohort study of 11 hospital networks, including consecutive adult patients admitted with AKI and cirrhosis in 2019. The etiology of AKI was adjudicated based on pre-specified clinical definitions (prerenal/hypovolemic AKI, hepatorenal syndrome [HRS-AKI], acute tubular necrosis [ATN], other).
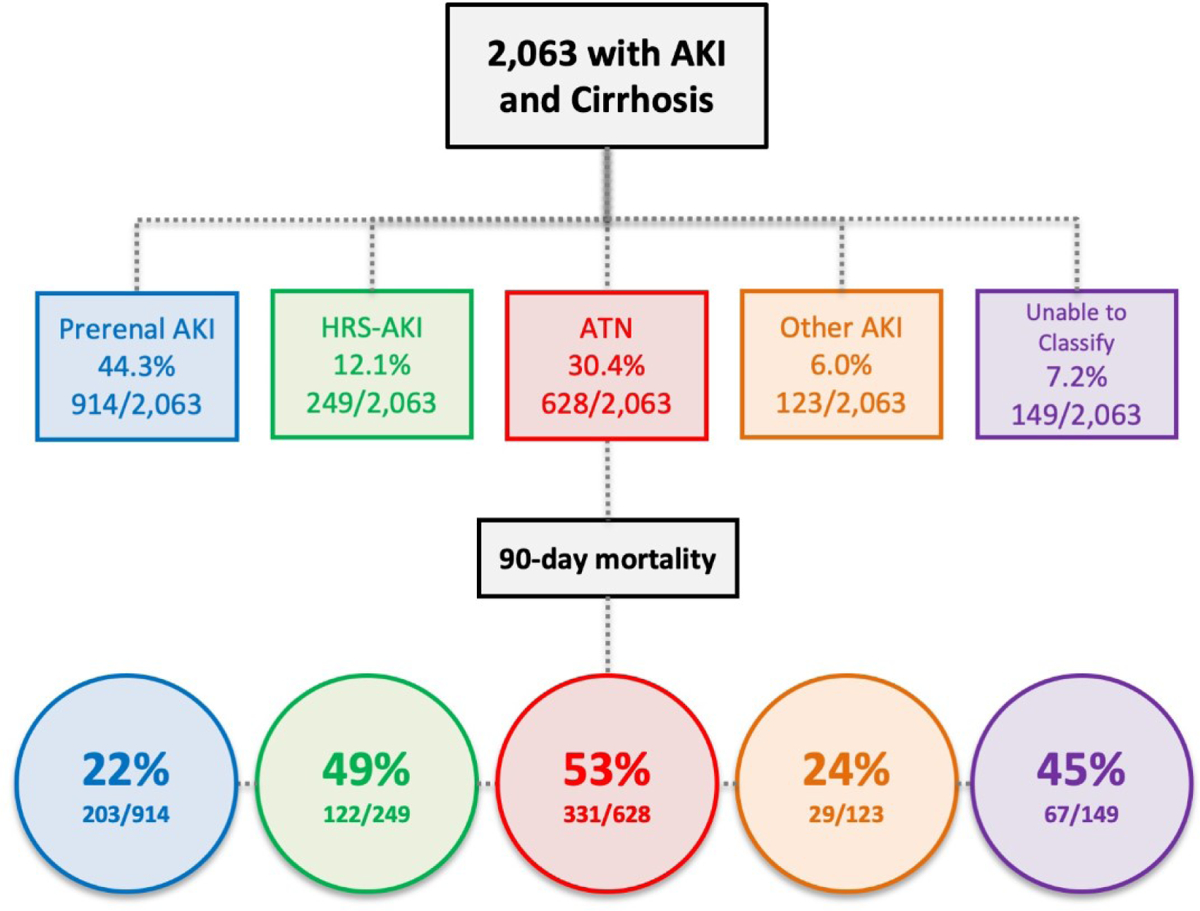
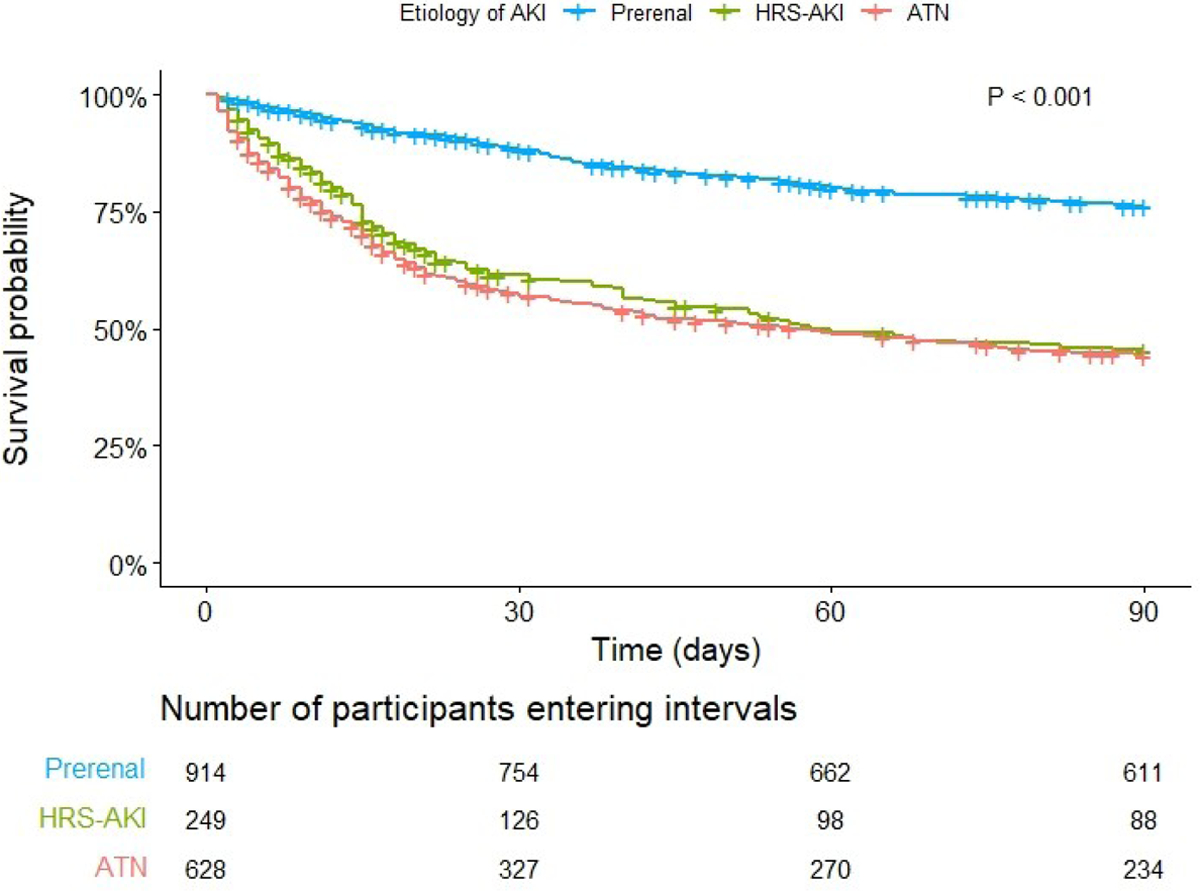
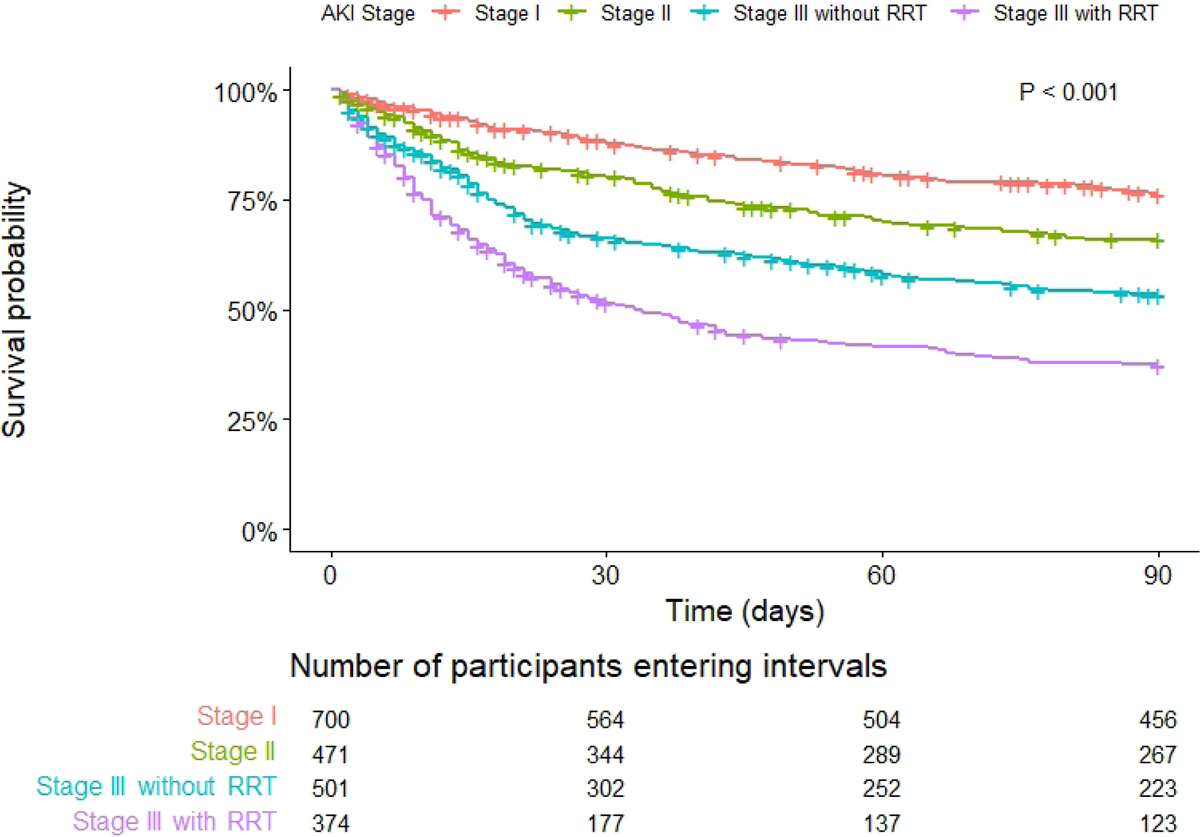
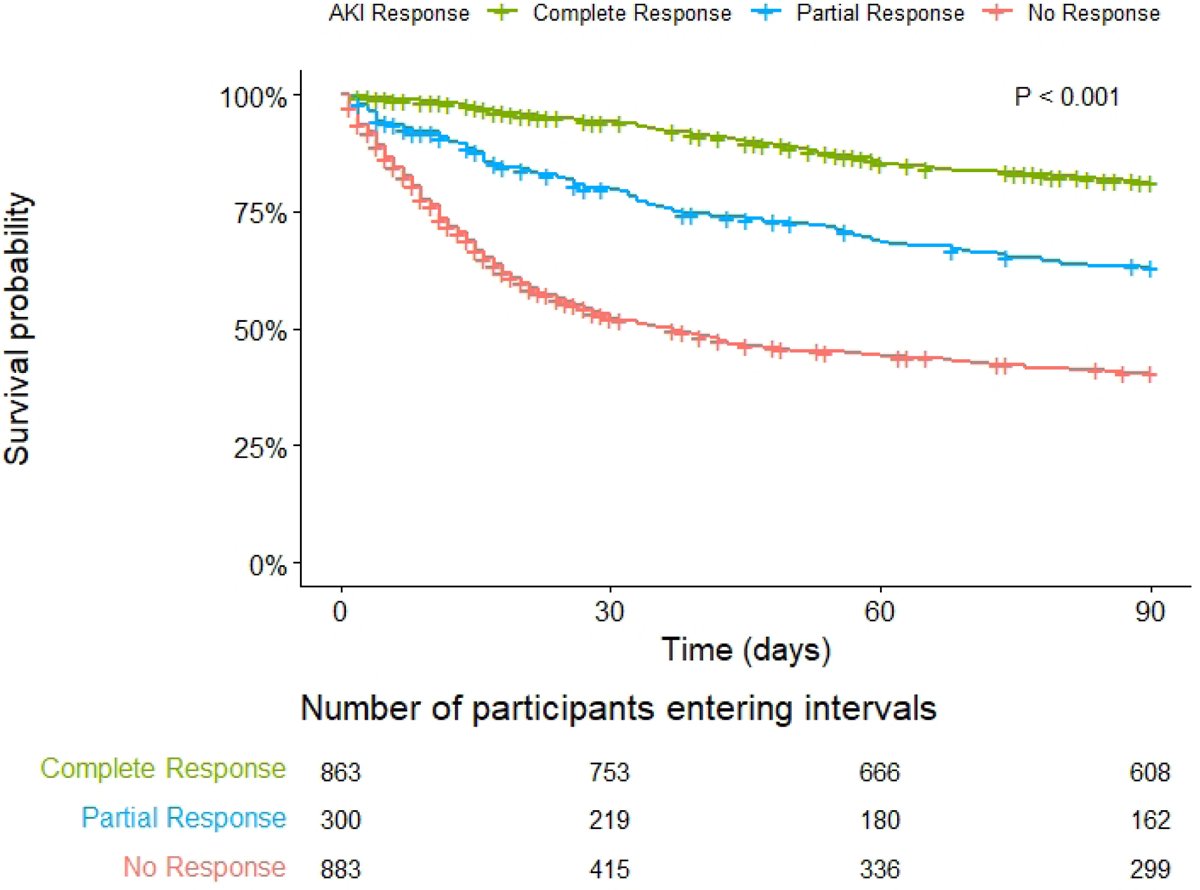
Results: A total of 2,063 patients were included (median age 62 [IQR 54-69] years, 38.3% female, median MELD-Na score 26 [19-31]). The most common etiology was prerenal AKI (44.3%), followed by ATN (30.4%) and HRS-AKI (12.1%); 6.0% had other AKI, and 7.2% could not be classified. In our cohort, 8.1% of patients received a liver transplant and 36.5% died by 90 days. The lowest rate of death was observed in patients with prerenal AKI (22.2%; p <0.001), while death rates were higher but not significantly different from each other in those with HRS-AKI and ATN (49.0% vs. 52.7%; p = 0.42). Using prerenal AKI as a reference, the adjusted subdistribution hazard ratio (sHR) for 90-day mortality was higher for HRS-AKI (sHR 2.78; 95% CI 2.18-3.54; p <0.001) and ATN (sHR 2.83; 95% CI 2.36-3.41; p <0.001). In adjusted analysis, higher AKI stage and lack of complete response to treatment were associated with an increased risk of 90-day mortality (p <0.001 for all).
Conclusion: AKI is a severe complication of cirrhosis. HRS-AKI is uncommon and is associated with similar outcomes to ATN. The etiology of AKI, AKI stage/severity, and non-response to treatment were associated with mortality. Further optimization of vasoconstrictors for HRS-AKI and supportive therapies for ATN are needed.
Impact and implications: Acute kidney injury (AKI) in cirrhosis carries high morbidity, and management is determined by the etiology of injury. However, a large and well-adjudicated multicenter database from US centers that uses updated AKI definitions is lacking. Our findings demonstrate that acute tubular necrosis and hepatorenal syndrome have similar outcomes (∼50% mortality at 90 days), though hepatorenal syndrome is uncommon (12% of all AKI cases). These findings represent practice patterns at US transplant/tertiary centers and can be used as a baseline, presenting the situation prior to the adoption of terlipressin in the US.
Keywords: acute on chronic liver failure; liver failure; liver transplant; renal failure; vasoconstrictor.
Copyright © 2023 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology (Baltimore, Md) 2008;48:2064–2077. - PubMed
-
- Angeli P, Gines P, Wong F, Bernardi M, Boyer TD, Gerbes A, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. Gut 2015;64:531–537. - PubMed
-
- Fagundes C, Barreto R, Guevara M, Garcia E, Sola E, Rodriguez E, et al. A modified acute kidney injury classification for diagnosis and risk stratification of impairment of kidney function in cirrhosis. Journal of hepatology 2013;59:474–481. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
