

S100A8∕A9 is a valuable biomarker and treatment target to detect and modulate neutrophil involvement in myocardial infarction
- PMID: 37518871
- PMCID: PMC10520380
- DOI: 10.47162/RJME.64.2.04
S100A8∕A9 is a valuable biomarker and treatment target to detect and modulate neutrophil involvement in myocardial infarction
Abstract
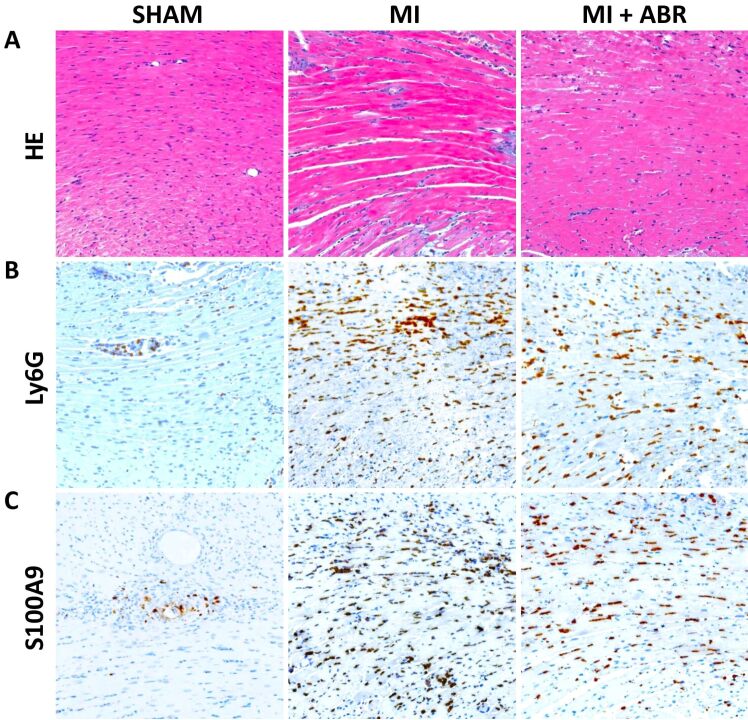
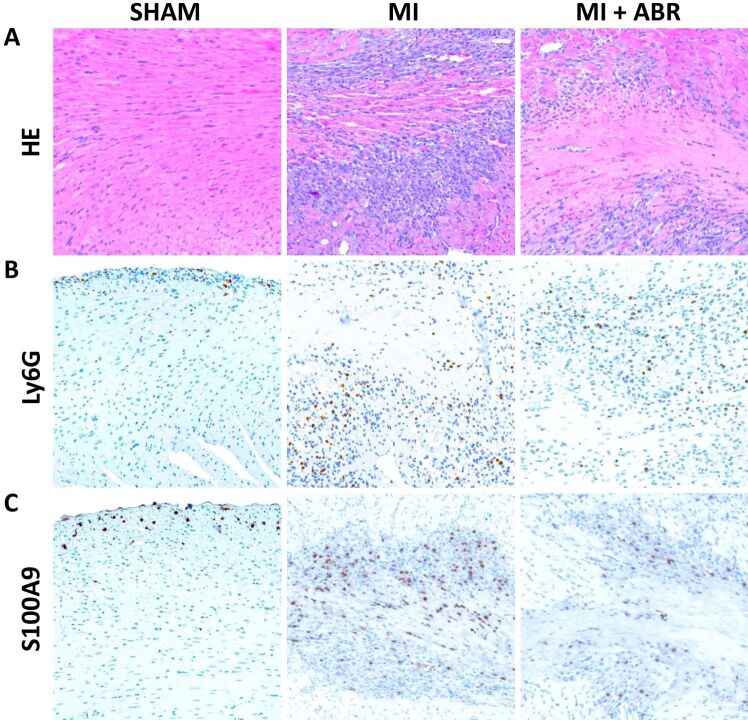
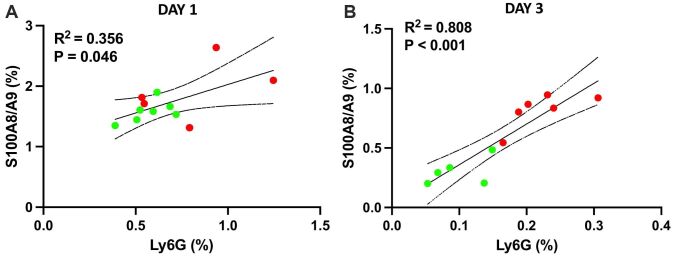
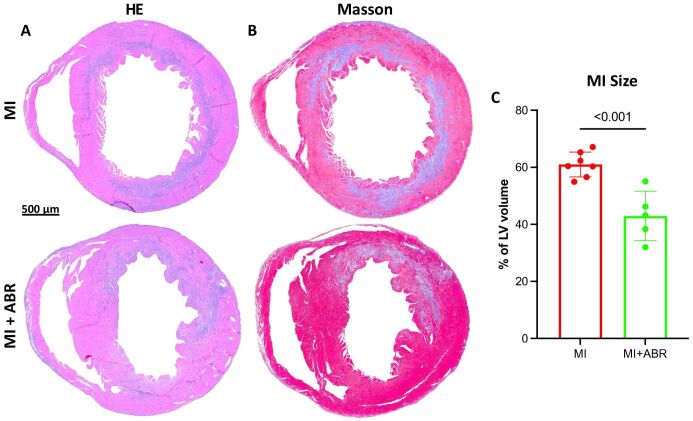
Myocardial infarction (MI) leads to irreversible ischemic damage of the heart muscle and is the leading cause of heart failure. The ischemic cardiac injury triggers a potent local and systemic immune response. In the acute phase post-MI, neutrophils infiltrate the myocardium in large numbers and induce further cardiomyocyte death, expanding the infarcted area. The alarmin S100A8∕A9 is a proinflammatory mediator primarily produced by myeloid cells, with an emerging role in MI. We previously demonstrated that short-term inhibition of S100A8∕A9 during the inflammatory phase of the immune response to MI improves long-term cardiac function. In the present study, we investigated the effects of S100A8∕A9 blockade on myocardial inflammation and post-ischemic myocardial injury in a mouse model of coronary artery ligation. Immunohistochemical (IHC) staining revealed that the presence of S100A9 is strongly correlated with neutrophil infiltration in the myocardium on days 1 and 3 post-MI. A 3-day treatment with the S100A8∕A9 blocker ABR-238901 starting immediately after MI decreased the number of neutrophils and S100A9 presence in the myocardium and had a positive impact on cardiac damage, reducing infarction size. These findings promote S100A9 as an IHC biomarker of neutrophil infiltration and a promising immunomodulatory target to regulate neutrophil recruitment, reduce ischemic injury and promote long-term beneficial cardiac recovery after MI.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures
References
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; Fourth universal definition of myocardial infarction (2018) J Am Coll Cardiol. 2018;72(18):2231–2264. - PubMed
-
- Mares RG, Marinkovic G, Cotoi OS, Schiopu A. Innate immune mechanisms in myocardial infarction – an update. Rev Rom Med Lab. 2018;26:9–20.
-
- Yan X, Anzai A, Katsumata Y, Matsuhashi T, Ito K, Endo J, Yamamoto T, Takeshima A, Shinmura K, Shen W, Fukuda K, Sano M. Temporal dynamics of cardiac immune cell accumulation following acute myocardial infarction. J Mol Cell Cardiol. 2013;62:24–35. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
