

Does Immediate Postoperative Early Ambulation Affect Clinical Results of Full-Endoscopic Lumbar Discectomy? A Historical Control Study of Daytime Operation with a 8-Hour Hospital Stay versus Inpatient Operation
- PMID: 37519265
- PMCID: PMC10475658
- DOI: 10.1111/os.13814
Does Immediate Postoperative Early Ambulation Affect Clinical Results of Full-Endoscopic Lumbar Discectomy? A Historical Control Study of Daytime Operation with a 8-Hour Hospital Stay versus Inpatient Operation
Abstract
Objective: Full-endoscopic lumbar discectomy (FELD) is a popular operation for the treatment of lumbar disc herniation (LDH) and day surgery mode is increasingly popular. However, only a few studies have reported about day surgery patients undergoing Percutaneous endoscopic lumbar discectomy (PELD). This retrospective study was to evaluate and analyze the clinical outcomes of patients undergoing FELD for LDH as day surgery versus inpatient surgery.
Methods: From January 2020 to January 2022, a retrospective analysis of LDH patients treated with FELD either in day surgery unit (within 8-h hospital stay) or inpatient unit was carried out. All these patients were followed-up for at least 12 months, and were categorized into a FELD-I (inpatient surgery) group or a FELD-D (day surgery) group, according to where the surgical procedures were performed. We assessed and compared the postoperative stand and walk time, postoperative hospitalization stays, time of return to work, modified MacNab criteria, willingness to recommend surgery, complications, revision rate, as well as the visual analogue scale (VAS) and the Oswestry disability index score (ODI). Student t-test was used for continuous variables and chi-square test or Fisher's exact test was used for categorical variables.
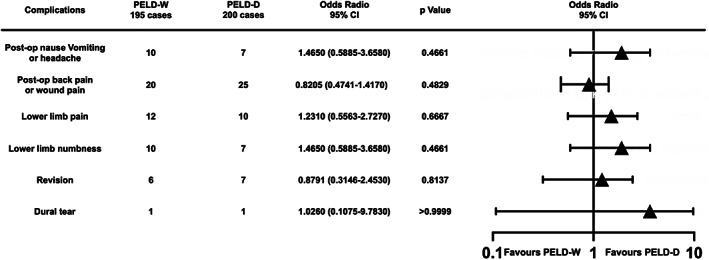
Results: There was no statistically significant difference in demographic data and baseline characteristics between two groups. And no significant differences were found in MacNab criteria between two groups. Postoperative VAS and ODI scores at one-day postoperation and final follow-up both improved significantly in both groups, as compared to the preoperative data (p < 0.001). However, no significant difference was found between the two groups on the pre, postoperative, or the last follow-up score for VAS and ODI (p > 0.05). The postoperative first ambulation time and postoperative hospital stays was much longer in FELD-I group than FELD-D group (p < 0.001). However, there were no significant differences in the perioperative complications, revision rate as well as satisfaction rate between two groups (p > 0.05). The overall time of return to work of young patients (<60 years-old) in the FELD-D group was significantly shorter than that in the FELD-I group (p = 0.001). Patients in the FELD-D group were more likely to recommend this kind of surgical model.
Conclusion: These data suggest that FELD-D can be effectively performed as day surgery (within 8 h hospital stay). Early ambulation after FELD-D did not affect the clinical outcomes and the revision rates. Day surgery patients are more likely to recommend this surgery mode to other patients and younger patients may be able to return to work earlier.
Keywords: Ambulation; Day surgery; Discectomy; Endoscopic; Lumbar disc herniation.
© 2023 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
