

The Radiological Spectrum of Rhino-Oculo-Cerebral Mucormycosis
- PMID: 37519552
- PMCID: PMC10374177
- DOI: 10.7759/cureus.40932
The Radiological Spectrum of Rhino-Oculo-Cerebral Mucormycosis
Abstract
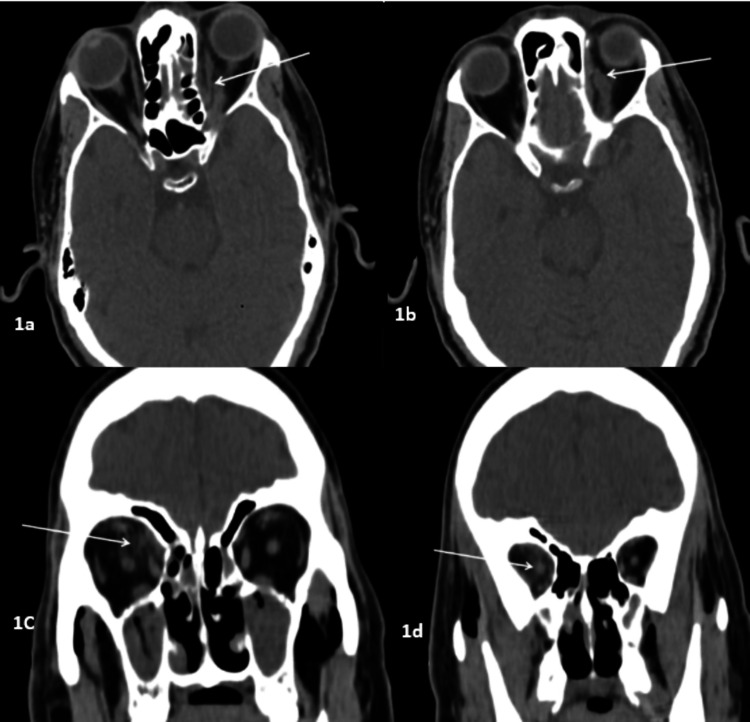
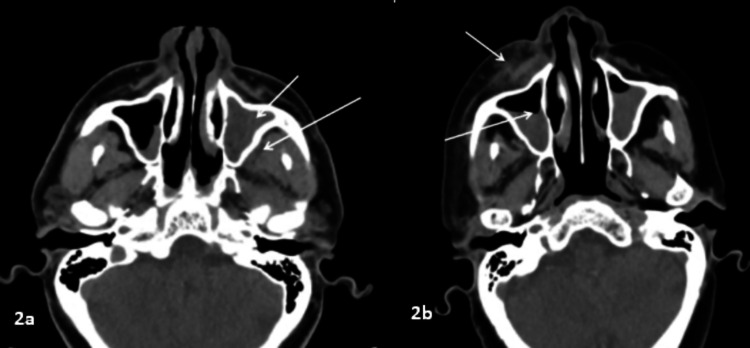
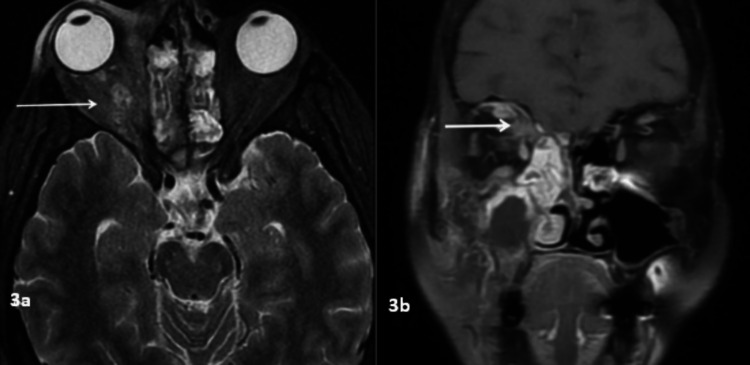
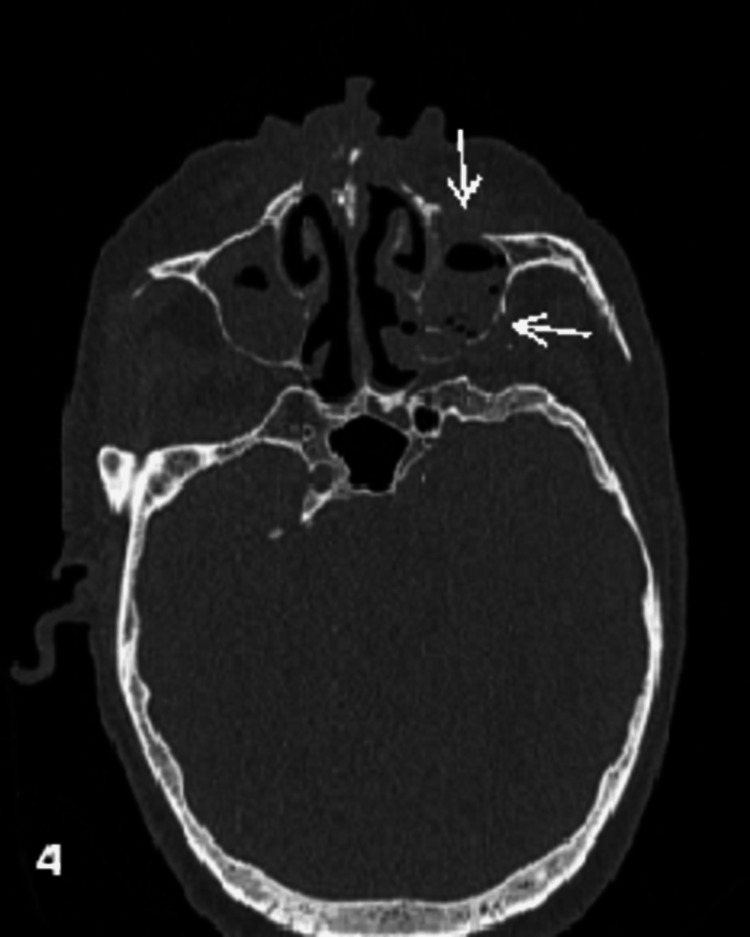
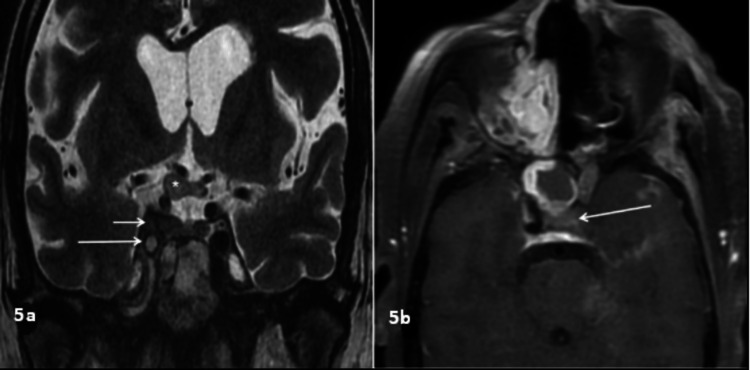
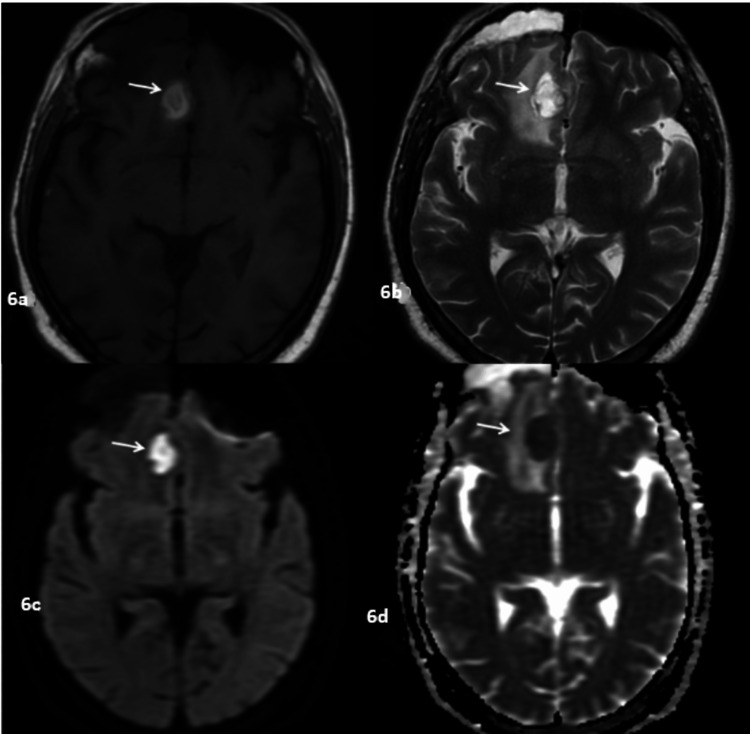
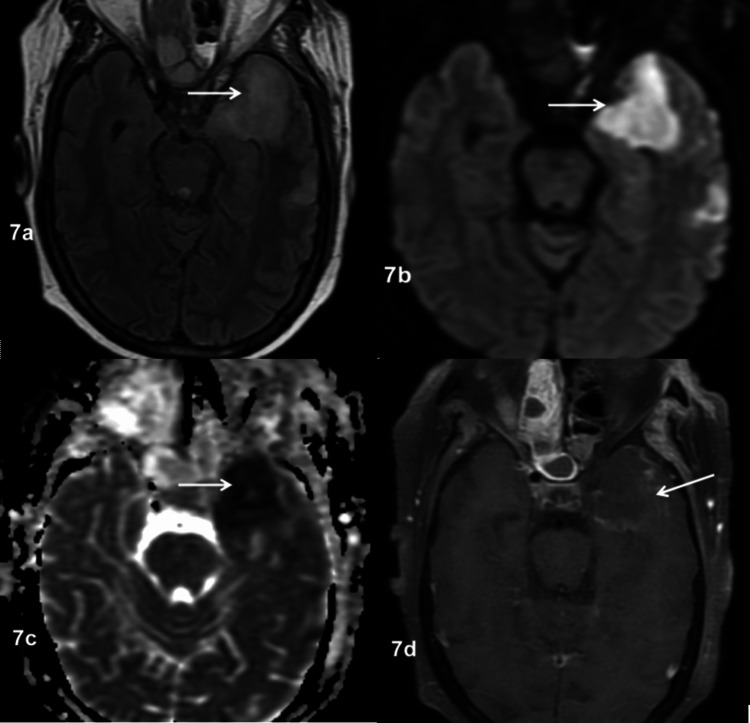
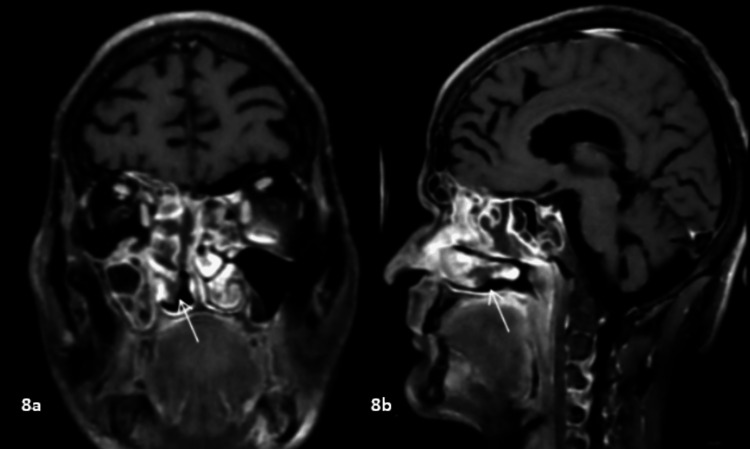
Aim We aim to study the spectrum of imaging findings in patients with rhino-oculo-cerebral mucormycosis (ROCM). Materials and methods This retrospective descriptive study was performed in histopathologically confirmed cases of rhino-oculo-cerebral mucormycosis in a tertiary care center in Bihar, India. The case records of patients with radiological, cultural, and histological evidence of acute invasive ROCM were retrospectively evaluated for relevant radiological and clinical data between May 2021 and June 2022. Results The radiological evaluation included computed tomography (CT) and magnetic resonance imaging (MRI) scans done on 52 patients. The patient's average age was 48 years. The ethmoid sinus was involved in 51 (98%) cases and the maxillary sinus in 50 (96%) cases. Bilateral sinus involvement (45, 86%) was the most common, followed by pansinus involvement (27, 52%). The orbit was involved in 39 (75%) cases, the face in 25 (47%) cases, and retroantral fat stranding in 24 (46%) cases. Mucosal thickening (91%) was the most common pattern of involvement, followed by complete opacification (77%). Osseous involvement was seen in 17 of 44 patients who had CT scans, and the majority of patients had extrasinus extension with intact bone. MRI revealed variable T2SI, with T2 hyperintensity being the most common pattern. Heterogeneous enhancement in post-contrast imaging was the most common. Conclusion ROCM is a life-threatening invasive fungal infection, especially in an immunocompromised state. ROCM is characterized by a variety of imaging abnormalities on CT and MRI, although nonspecific. Imaging aids in suspicion or early diagnosis in appropriate clinical contexts, particularly in an immunocompromised state, and in determining the degree of involvement and complications. Early detection of ROCM and its complications enables proper treatment, which can lower the cost of care, morbidity, and mortality.
Keywords: fungal; mucormycosis infection; paranasal sinus; radiological spectrum; rhino-oculo-cerebral mucormycosis; rocm.
Copyright © 2023, . et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Imaging features of invasive and noninvasive fungal sinusitis: a review. Aribandi M, McCoy VA, Bazan C 3rd. https://doi.org/10.1148/rg.275065189. Radiographics. 2007;27:1283–1296. - PubMed
-
- Imaging features of rhinocerebral mucormycosis: a study of 43 patients. Therakathu J, Prabhu S, Irodi A, Sudhakar SV, Yadav VK, Rupa V. https://doi.org/10.1016/j.ejrnm.2018.01.001 Egypt J Radiol Nucl Med. 2018;49:447–452.
-
- Epidemiology and clinical manifestations of mucormycosis. Petrikkos G, Skiada A, Lortholary O, Roilides E, Walsh TJ, Kontoyiannis DP. http://dx.doi.org/10.1093/cid/cir866. Clin Infect Dis. 2012;54:0–34. - PubMed
LinkOut - more resources
Full Text Sources