

Association analysis between symptomology and herpesvirus IgG antibody concentrations in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and multiple sclerosis
- PMID: 37519635
- PMCID: PMC10372404
- DOI: 10.1016/j.heliyon.2023.e18250
Association analysis between symptomology and herpesvirus IgG antibody concentrations in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and multiple sclerosis
Abstract
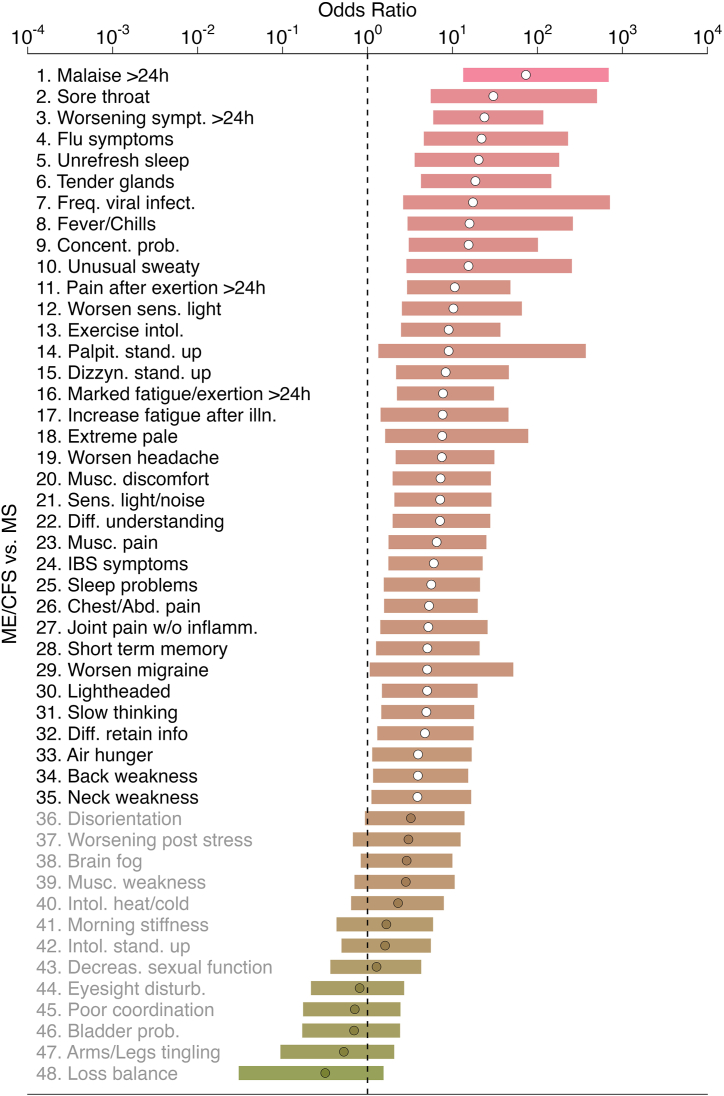
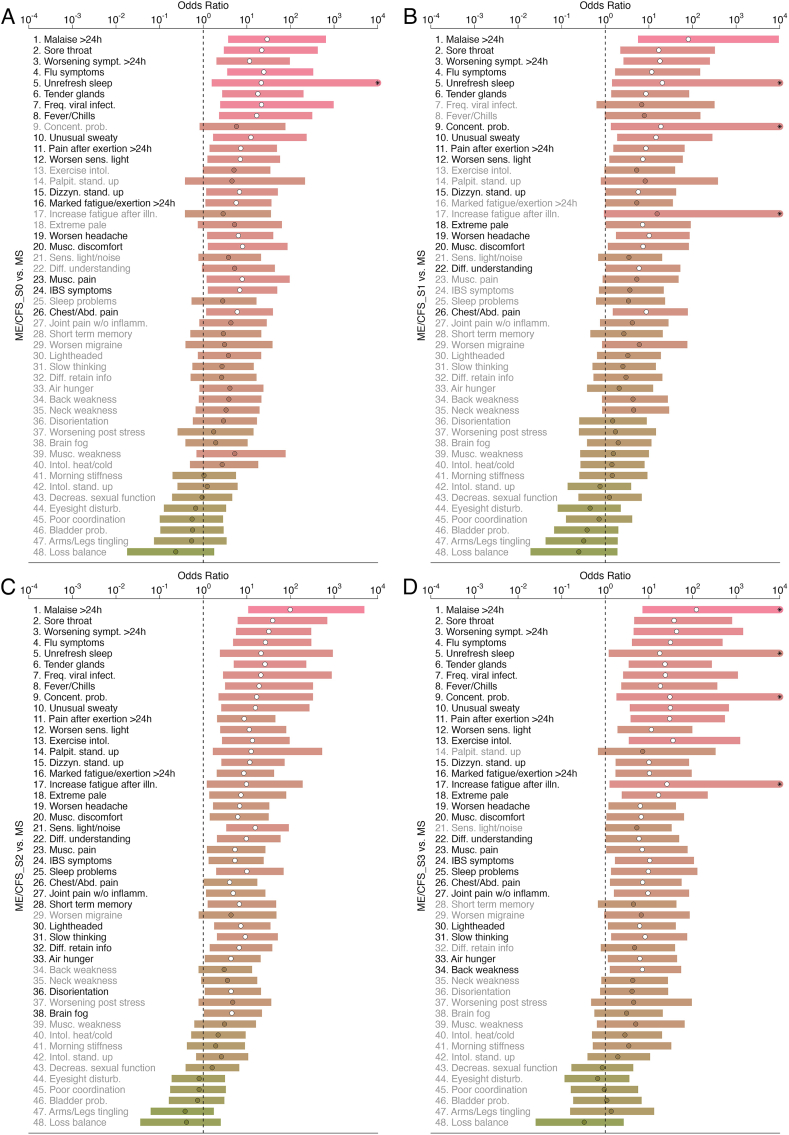
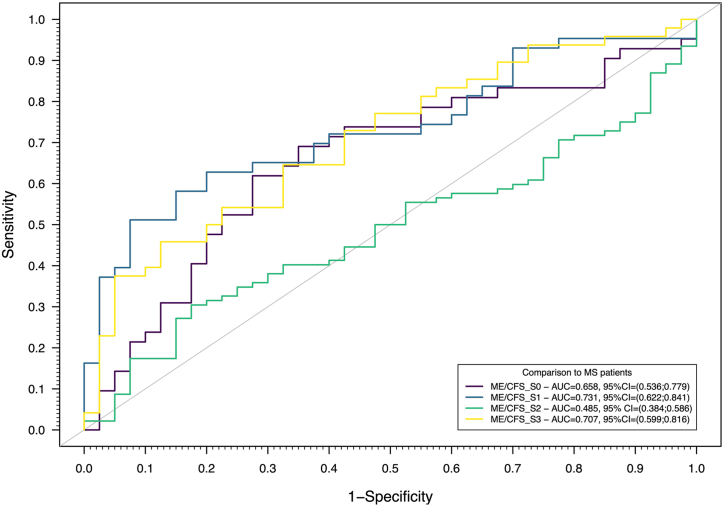
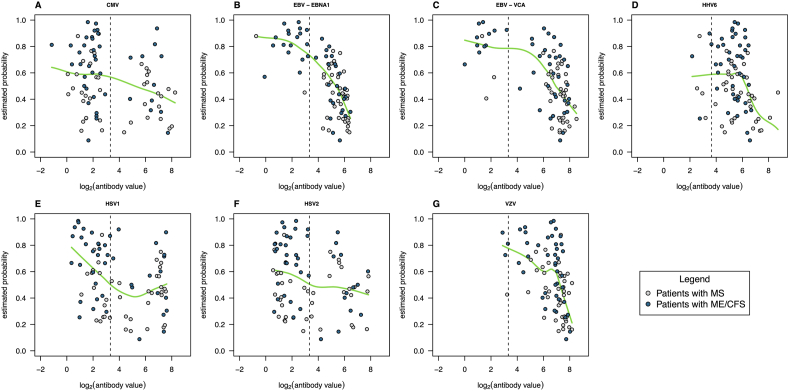
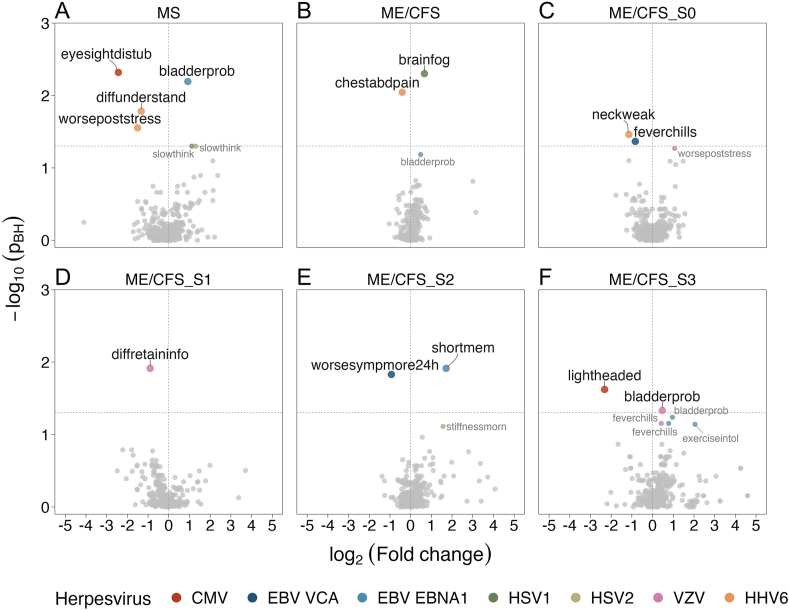
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and multiple sclerosis (MS) are two complex and multifactorial diseases whose patients experience persistent fatigue, cognitive impairment, among other shared symptoms. The onset of these diseases has also been linked to acute herpesvirus infections or their reactivations. In this work, we re-analyzed a previously-described dataset related to IgG antibody responses to 6 herpesviruses (CMV - cytomegalovirus; EBV - Epstein-Barr virus; HHV6 - human herpesvirus-6; HSV1 and HSV2 - herpes simplex virus-1 and -2, respectively; VZV - varicella-zoster virus) from the United Kingdom ME/CFS biobank. The primary goal was to report the underlying symptomology and its association with herpesvirus IgG antibodies using data from 4 disease-trigger-based subgroups of ME/CFS patients (n = 222) and patients with MS (n = 46). The secondary objective was to assess whether serological data could distinguish ME/CFS and its subgroup from MS using a SuperLearner (SL) algorithm. There was evidence for a significant negative association between temporary eye insight disturbance and CMV antibody concentrations and for a significant positive association between bladder problems and EBV antibody concentrations in the MS group. In the ME/CFS or its subgroups, the most significant antibody-symptom association was obtained for increasing HSV1 antibody concentration and brain fog, a finding in line with a negative impact of HSV1 exposure on cognitive outcomes in both healthy and disease conditions. There was also evidence for a higher number of significant antibody-symptom associations in the MS group than in the ME/CFS group. When we combined all the serological data in an SL algorithm, we could distinguish three ME/CFS subgroups (unknown disease trigger, non-infection trigger, and an infection disease trigger confirmed in the lab at the time of the event) from the MS group. However, we could not find the same for the remaining ME/CFS group (related to an unconfirmed infection disease). In conclusion, IgG antibody data explains more the symptomology of MS patients than the one of ME/CFS patients. Given the fluctuating nature of symptoms in ME/CFS patients, the clinical implication of these findings remains to be determined with a longitudinal study. This study is likely to ascertain the robustness of the associations during natural disease course.
Keywords: Cytomegalovirus; Enzyme-linked immunosorbent assay; Epstein-barr virus; Herpes simplex virus-1 and -2; Human herpesvirus-6; SuperLearner; United Kingdom ME/CFS biobank; Varicella-zoster virus.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Scheibenbogen C., Freitag H., Blanco J., Capelli E., Lacerda E., Authier J., Meeus M., Castro Marrero J., Nora-Krukle Z., Oltra E., Strand E.B., Shikova E., Sekulic S., Murovska M. The European ME/CFS Biomarker Landscape project: an initiative of the European network EUROMENE. J. Transl. Med. 2017;15:162. doi: 10.1186/s12967-017-1263-z. - DOI - PMC - PubMed
-
- Nacul L., Authier F.J., Scheibenbogen C., Lorusso L., Helland I.B., Martin J.A., Sirbu C.A., Mengshoel A.M., Polo O., Behrends U., Nielsen H., Grabowski P., Sekulic S., Sepulveda N., Estévez-López F., Zalewski P., Pheby D.F.H., Castro-Marrero J., Sakkas G.K., Capelli E., Brundsdlund I., Cullinan J., Krumina A., Bergquist J., Murovska M., Vermuelen R.C.W., Lacerda E.M. European network on myalgic encephalomyelitis/chronic fatigue syndrome (EUROMENE): expert Consensus on the diagnosis, Service provision, and care of people with ME/CFS in europe. Medicina (Kaunas) 2021;57:510. doi: 10.3390/medicina57050510. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
