

Pediatric diencephalic tumors: a constellation of entities and management modalities
- PMID: 37519792
- PMCID: PMC10374860
- DOI: 10.3389/fonc.2023.1180267
Pediatric diencephalic tumors: a constellation of entities and management modalities
Abstract
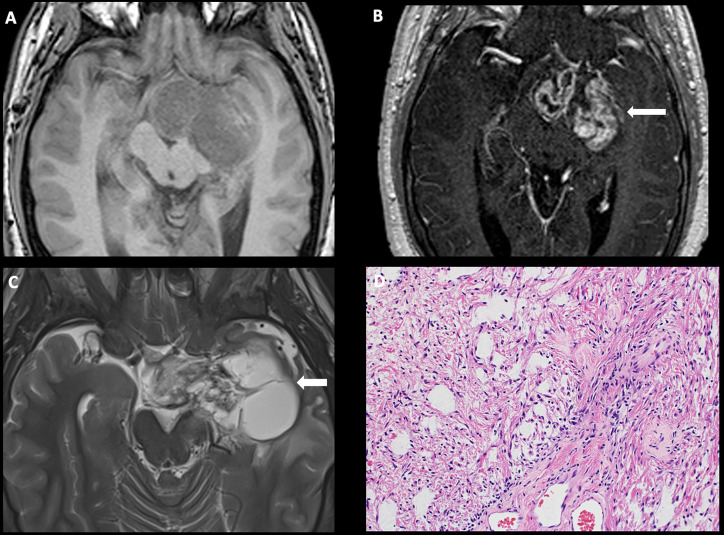
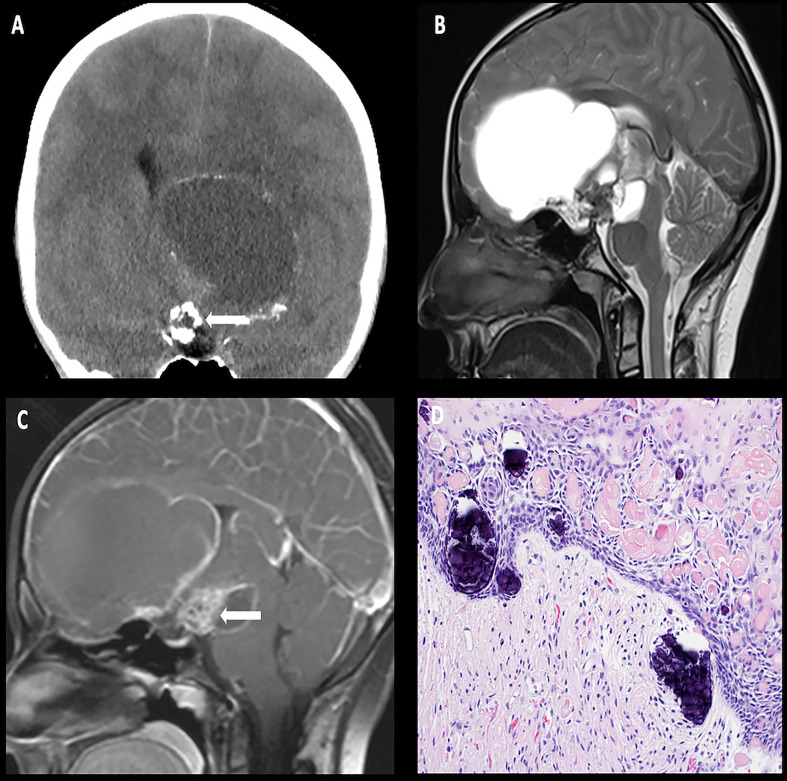
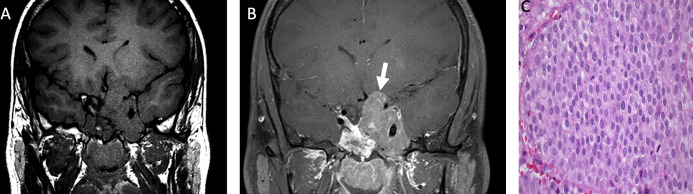
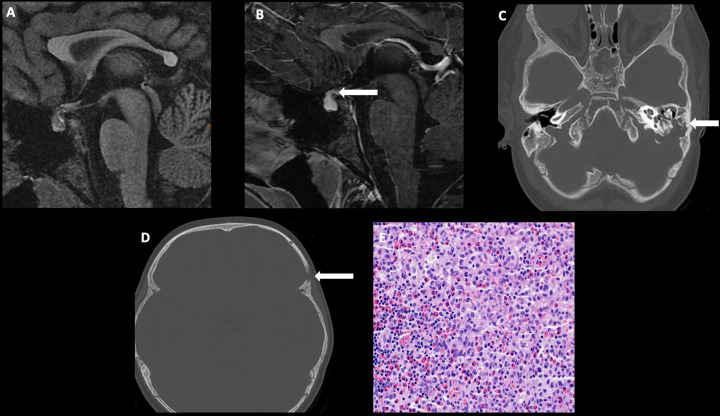
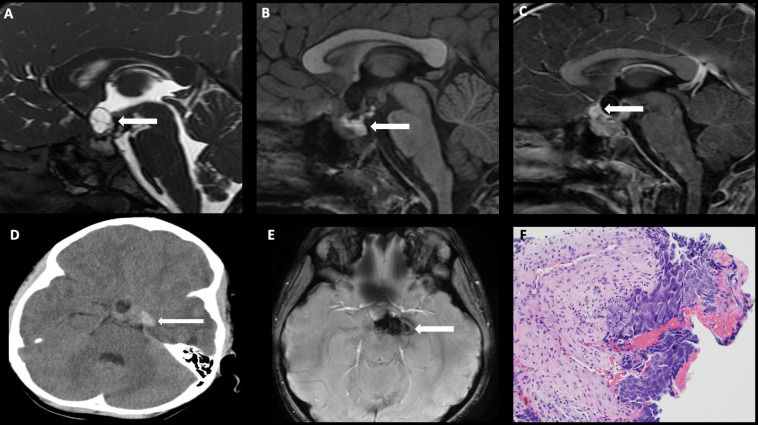
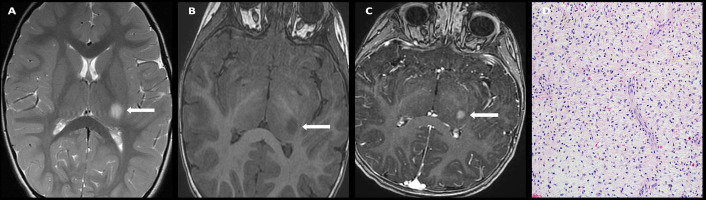
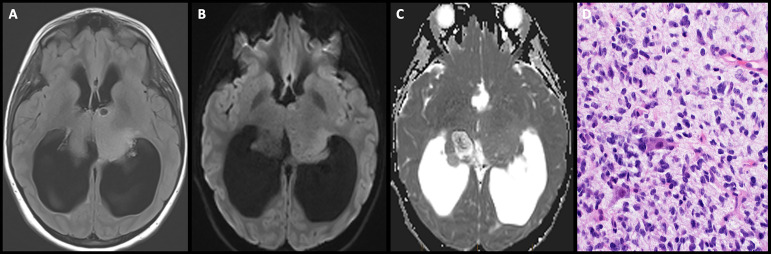
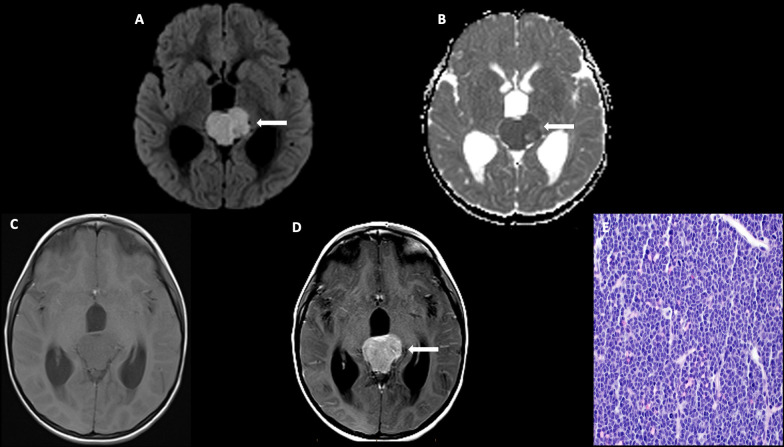
The diencephalon is a complex midline structure consisting of the hypothalamus, neurohypophysis, subthalamus, thalamus, epithalamus, and pineal body. Tumors arising from each of these diencephalic components differ significantly in terms of biology and prognosis. The aim of this comprehensive review is to describe the epidemiology, clinical symptoms, imaging, histology, and molecular markers in the context of the 2021 WHO classification of central nervous system neoplasms. We will also discuss the current management of each of these tumors.
Keywords: adenoma; craniopharyngioma; diencephalon; germ cell tumor; langerhans cell histiocytosis; pineoblastoma.
Copyright © 2023 Pinto, Chiang, Qaddoumi, Livingston and Bag.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources