

Cardiac Masses Discovered by Echocardiogram; What to Do Next?
- PMID: 37520139
- PMCID: PMC10382990
- DOI: 10.1016/j.shj.2022.100154
Cardiac Masses Discovered by Echocardiogram; What to Do Next?
Abstract
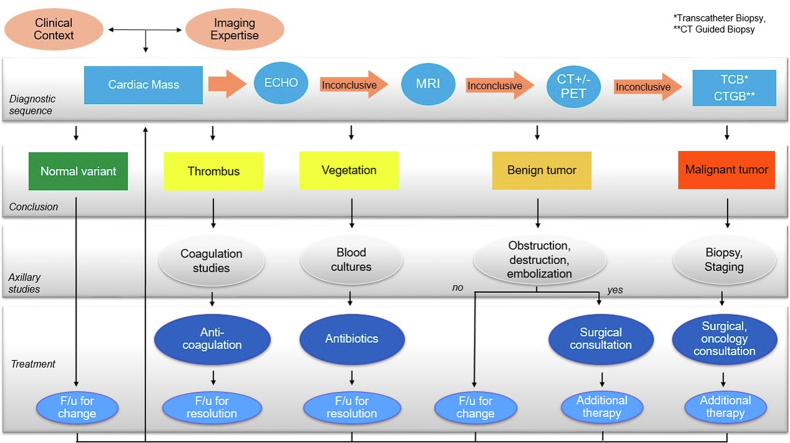
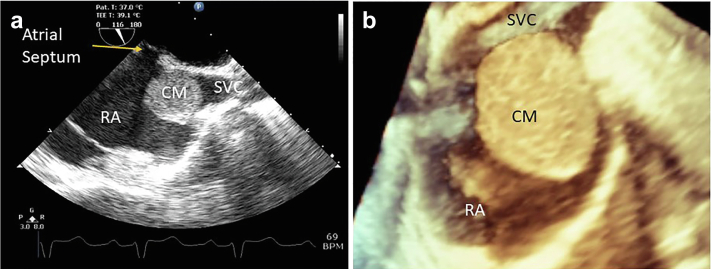
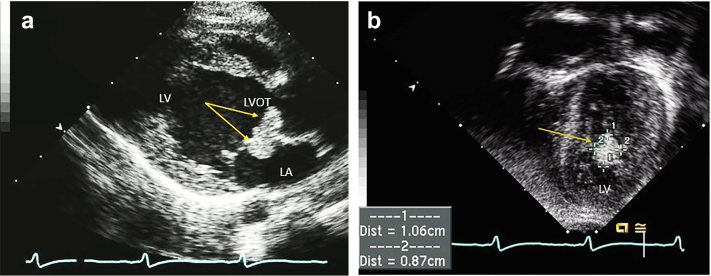
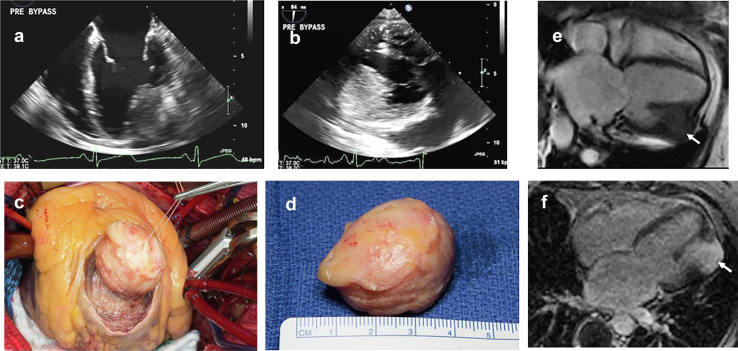
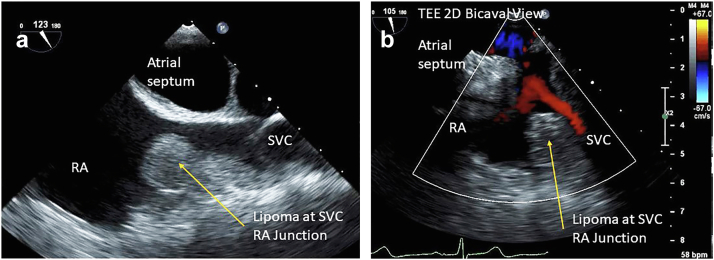
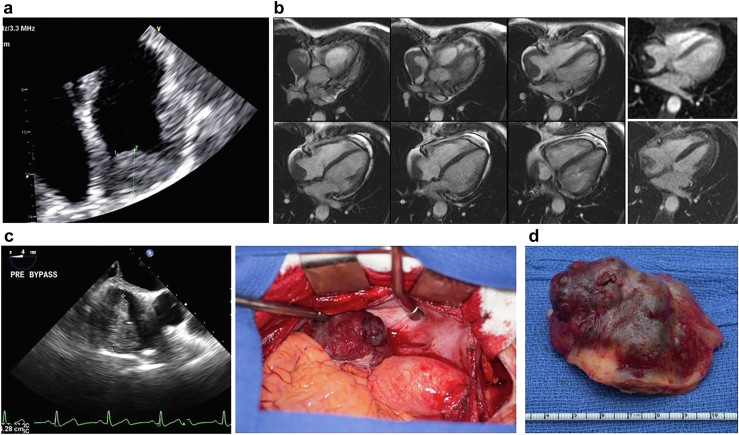
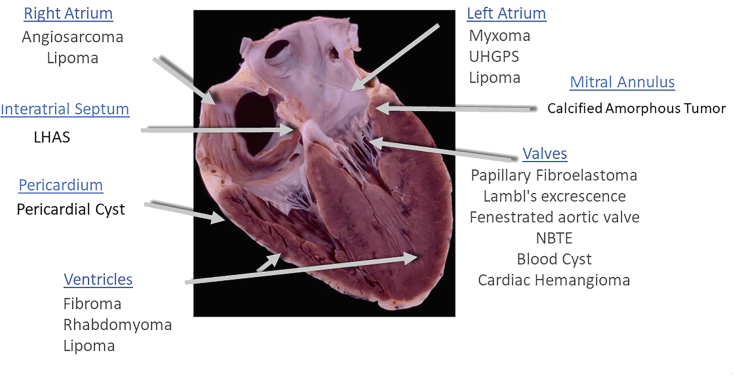
Cardiac tumors are rare conditions, typically diagnosed on autopsy, but with the advancement of imaging techniques they are now encountered more frequently in clinical practice. Echocardiography is often the initial method of investigation for cardiac masses and provides a quick and valuable springboard for their characterization. While some cardiac masses can be readily identified by echocardiography alone, several require incorporation of multiple data points to reach diagnostic certainty. Herein, we will provide an overview of the main clinical, diagnostic, and therapeutic characteristics of cardiac masses within the framework of their location.
Keywords: Cardiac computed tomography; Cardiac magnetic resonance; Cardiac masses; Cardiac tumors; Echocardiography; Multimodality imaging; Myxoma; NBTE; Papillary fibroelastoma; Primary tumors.
© 2023 The Authors.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- Bruce C.J. Cardiac tumours: diagnosis and management. Heart. 2011;97:151–160. - PubMed
-
- Al-Mamgani A., Baartman L., Baaijens M., de Pree I., Incrocci L., Levendag P.C. Cardiac metastases. Int J Clin Oncol. 2008;13:369–372. - PubMed
-
- Reynen K., Kockeritz U., Strasser R.H. Metastases to the heart. Ann Oncol. 2004;15:375–381. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
