

Hospital stays and costs of telemedical monitoring versus standard follow-up for diabetic foot ulcer: an open-label randomised controlled study
- PMID: 37520145
- PMCID: PMC10384180
- DOI: 10.1016/j.lanepe.2023.100686
Hospital stays and costs of telemedical monitoring versus standard follow-up for diabetic foot ulcer: an open-label randomised controlled study
Abstract
Background: Two randomised controlled trials (RCTs) have previously shown that telemedical monitoring of diabetic foot ulcer (DFU) reduces the number of visits to the outpatient clinic, without losing treatment efficacy or increasing costs. Here we present the results of an open-label, randomised controlled trial designed to investigate whether telemonitoring, provided by an expert nurse (with extensive experience in DFU and trained in remote monitoring), reduces the hospital stay and the associated costs for a patient with DFU (TELEPIED trial).
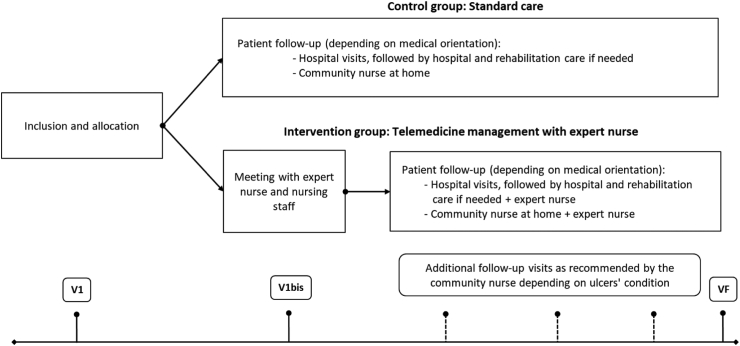
Methods: Eligible patients (n = 180) were randomly allocated to: (i) a control group, in which they received standard care, and (ii) an intervention group, in which they received asynchronous telemedicine follow-up by the expert nurse. The primary outcome was the cumulative hospital days over 12 months. The main secondary outcomes were (i) direct healthcare costs (estimated in a collective perspective), (ii) wound healing and (iii) amputation rates. ITT (intention-to-treat) population was analysed.
Findings: In the ITT population, cumulative hospital days were significantly higher in the control group (13.4 days [95% CI 9.0-17.8]) than in the intervention group (7.1 days [2.8-11.5]) (p = 0.0458, ANCOVA model). Cumulative direct costs over 12 months were 7185 € (95% CI 5144-9226) in the control group and 3471 € (95% CI 1430-5512) in the intervention group (p = 0.0120). The percentage of wounds healed and amputation rate were not significantly different between groups. Similar results were found with the PP population.
Interpretation: The implementation of a telemedical intervention with an expert nurse could lead to a length of hospitalization and direct costs that were two times lower compared to conventional follow-up. This lower medical and economic burden was obtained without losing effectiveness on the rate of healing, nor increasing the amputation rate. Additional studies are required to confirm these findings.
Funding: This study was designed, funded and conducted by CERITD (Study and Research Centre for Intensification of Diabetes Treatment, Evry, France), Genopole GIP, 20 rue Henri Desbruères, 91030 EVRY Cedex and Laboratoires URGO, 15 Avenue d'Iéna, 75116 Paris Cedex, France. The findings and conclusions in this study are those of the authors and do not necessarily represent the views of the sponsor. The corresponding author (DD) certify that authors were not precluded from accessing data in the study, and they accept responsibility to submit for publication.
Keywords: Clinical trial; Diabetes; Diabetes complications; Diabetic foot ulcer; Expert nurse; Health cost; Hospitalization; Telehealth; Telemedicine.
© 2023 The Authors.
Conflict of interest statement
DD has received personal compensation for board participation and speaking fees from Sanofi and Urgo. SF has received personal compensation for board participation and speaking fees from Novo Nordisk, Roche Diagnostics, Lifescan, Sanofi, Diabeloop and Eli Lilly, received Research support from MSD and is employed by CERITD and is a shareholder of Diabeloop. GC is employed by CERITD and received personal compensation for board participation, research funding, and speaking fees from Astra-Zeneca, Boehringer, Eli Lilly, Johnson & Johnson, MSD, Novo-Nordisk, Sanofi-Aventis and Voluntis. LO and EB are employed by CERITD.MB has no conflict of interest to declare. IX was employed by CERITD. ZA (Zohra Amrous) is employed by CERITD.KLS has no conflict of interest to declare. BD was employed by Cemka, a consulting team specializing in health economics, epidemiology, and outcomes research. BD also received personal compensation for board participation and speaking fees from MSD, Novo-Nordisk, Sanofi, Eli Lilly, Janssen and Pfizer. AP received personal compensation for board participation and speaking fees from Abbott, Ascencia, Astra-Zeneca, Eli Lilly, Medtronic, MSD, Novartis, Novo Nordisk and Sanofi Aventis.
Figures

References
-
- Oliver T.I., Mutluoglu M. StatPearls Publishing; 2022. Diabetic foot ulcer.https://www.ncbi.nlm.nih.gov/books/NBK537328/ - PubMed
-
- Sorber R., Abularrage C.J. Diabetic foot ulcers: epidemiology and the role of multidisciplinary care teams. Semin Vasc Surg. 2021;34(1):47–53. - PubMed
-
- Armstrong D.G., Boulton A.J.M., Bus S.A. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367–2375. - PubMed
-
- Margolis D.J., Malay D.S., Hoffstad O.J., et al. Data Points Publication Series; Rockville (MD): 2011. Economic burden of diabetic foot ulcers and amputations: data Points #3. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
