

Effect of finger rest positions on upper limb muscle activity during pre-clinical procedures
- PMID: 37520265
- PMCID: PMC10386821
- DOI: 10.7717/peerj.15663
Effect of finger rest positions on upper limb muscle activity during pre-clinical procedures
Abstract
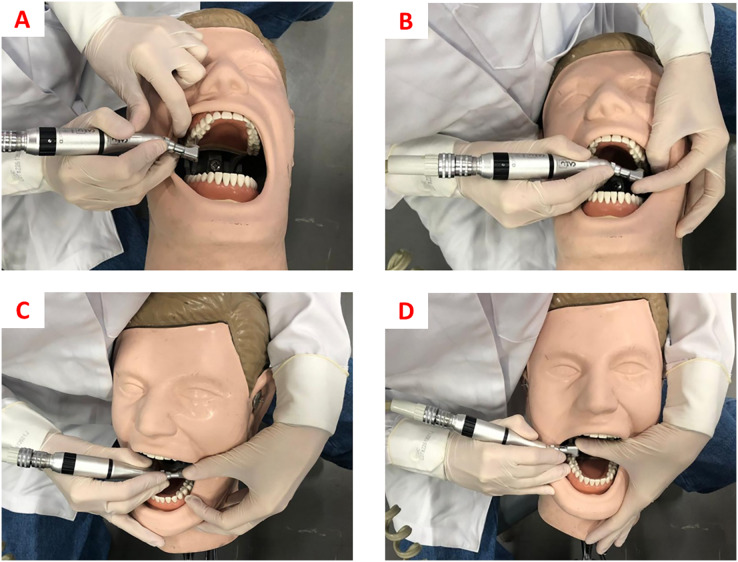
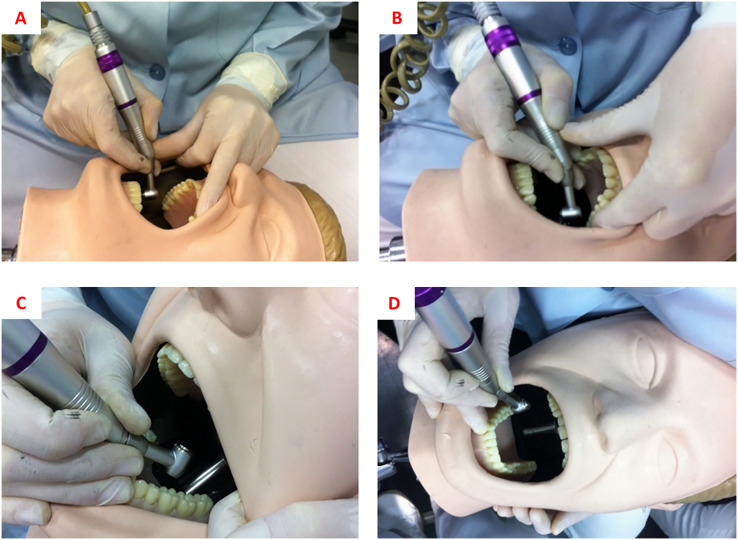
Objectives: This study aimed to observe the effect of different finger rest positions on the muscular activity of the hand, forearm, arm, shoulder, thorax, and neck, as well as on the angular deviation from the neutral position of the neck, trunk, upper arm, and forearm on the working side during pre-clinical procedures.
Methods: An experimental laboratory study was performed. Response variables were muscle activation of the abductor pollicis, brachioradialis, biceps brachii, deltoid, pectoralis major, and right sternocleidomastoid muscles and angular deviation from the neutral position of the neck, trunk, arm, and forearm during simulated clinical procedures. Independent variable was finger-rest position during cavity preparation (no finger rest, usual rest, and ergonomic rest). Class I cavity preparations (N = 120) were performed on artificial first molars (16, 26, 36, and 46) (N = 120). Muscular activation was assessed by surface electromyography and angular deviations using Software for Postural Assessment (SAPO) version 0.69. One-way analysis of variance and Tukey's or Games-Howell's post-hoc tests were performed (α = 0.05).
Results: For the sternocleidomastoid muscle, there was no statistically significant difference between the different rest positions. For the deltoid muscle, work with no finger rest resulted in greater muscle activation (p < 0.001) during work on tooth 36. Regarding the pectoralis major and right brachioradialis muscles, we observed that for both teeth 16 and 26, working with ergonomic rest showed less muscle activation. Muscle activation of the right biceps brachii was higher for work with no rest in both the upper and lower arches, differing significantly only from the usual rest in tooth 16 (p < 0.001), usual rest and ergonomic rest in teeth 26 and 46 (p < 0.001), and only ergonomic rest in tooth 36 (p = 0.044). In the right abductor pollicis muscle, work with ergonomic rest resulted in less muscle activation for cavity preparation in teeth 16, 26, and 36, which was significantly different from work with no rest (p = 0.029, p < 0.001, and p = 0.013, respectively). Regarding angular deviation, it was observed that for tooth 16, there was a greater angular deviation of the arm when performing cavity preparations with no finger rest. For teeth 26 and 46, the ergonomic finger rest provided lower angular deviation from the neutral position of the right arm. For tooth 36, ergonomic rest provided less angular deviation from the neutral neck position.
Conclusion: In general, the use of non-active finger rest during simulated cavity preparations, regardless of the type of rest, provided less muscle activation and angular deviation from the neutral position of the body's upper extremity when performing pre-clinical procedures.
Keywords: Dental students; Dentistry; Electromyography; Ergonomics; Finger rest position; Occupational health.
© 2023 Margato Pazos et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Alhazzazi TY, Alzebiani NA, Alotaibi SK, Bogari DF, Bakalka GT, Hazzazi LW, Jan AM, McDonald NJ. Awareness and attitude toward using dental magnification among dental students and residents at King Abdulaziz University, Faculty of Dentistry. BMC Oral Health. 2016;17(1):21. doi: 10.1186/s12903-016-0254-4. - DOI - PMC - PubMed
-
- Arnett MC, Gwozdek AE, Ahmed S, Beaubien HD, Yaw KB, Eagle IT. Assessing the use of loupes and lights in dental hygiene educational programs. Journal of Dental Hygiene. 2017;91(6):15–20. - PubMed
LinkOut - more resources
Full Text Sources
