

Racial/ethnic disparities in the distribution and effect of type and number of high-risk criteria on mortality in prostate cancer patients treated with radiotherapy
- PMID: 37521449
- PMCID: PMC10373609
- DOI: 10.1080/2090598X.2022.2148867
Racial/ethnic disparities in the distribution and effect of type and number of high-risk criteria on mortality in prostate cancer patients treated with radiotherapy
Abstract
Objective: To assess differences in the distribution of type and number of D'Amico high-risk criteria (DHRCs) according to race/ethnicity (R/E) and their effect on cancer-specific mortality (CSM) in prostate cancer (PCa) patients treated with external beam radiotherapy (RT).
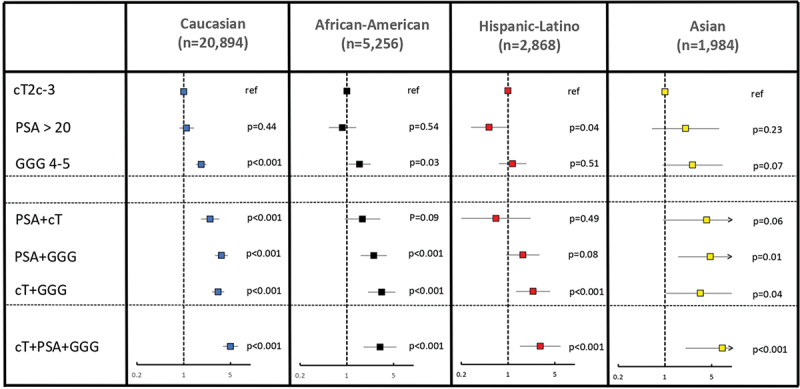
Methods: In the SEER database (2004-2016), we identified 31,002 PCa patients treated with RT with at least one DHRCs, namely PSA >20 ng/dL, biopsy Gleason Grade Group 4-5, and clinical T stage ≥T2c. Competing risks regression (CRR) model tested the association between DHRCs and 5-year CSM in all R/E subgroups.
Results: Of 31,002 patients, 20,894 (67%) were Caucasian, 5256 (17%) were African American, 2868 (9.3%) were Hispanic-Latino, and 1984 (6.4%) were Asian. The distributions of individual DHRCs and combinations of two DHRCs differed according to R/E, but not for the combination of three DHRCs. The effect related to the presence of a single DHRC, and combinations of two or three DHRCs on absolute CSM rates was lowest in Asians (1.2-6.8%), followed by in African Americans (2.3-12.2%) and Caucasians (2.3-12.1%), and highest in Hispanic/Latinos (1.7-13.8%). However, the opposite effect was observed in CRR, where hazard ratios were highest in Asians vs. other R/Es: Asians 1.00-2.59 vs. others 0.5-1.83 for one DHRC, Asians 3.4-4.75 vs. others 0.66-3.66 for two DHRCs, and Asians 7.22 vs. others 3.03-4.99 for all three DHRCs.
Conclusions: R/E affects the proportions of DHRCs. Moreover, within the four examined R/E groups, the effect of DHRCs on absolute and relative CSM metrics also differed. Therefore, R/E-specific considerations may be warranted in high-risk PCa patients treated with RT.
Keywords: CSM; D’Amico high-risk criteria; SEER; race/ethnicity; radiotherapy.
© 2022 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group.
Conflict of interest statement
The research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Av DA, W R, Sb M, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998. August;280(11):969–974. - PubMed
-
- van den Bergh R, Gandaglia G, Tilki D, et al. Trends in radical prostatectomy risk group distribution in a European multicenter analysis of 28 572 patients: towards tailored treatment. Eur Urol Focus. 2019. March;5(2):171–178. - PubMed
-
- Mahal BA, Berman RA, Taplin ME, et al. Prostate cancer-specific mortality across Gleason scores in black vs nonblack men. JAMA. 2018. December;320(23):2479–2481. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous