

Youth with severe mental illness and complex non-somatic motor abnormalities: conflicting conceptualizations and unequal treatment
- PMID: 37521496
- PMCID: PMC9533273
- DOI: 10.1038/s44184-022-00013-8
Youth with severe mental illness and complex non-somatic motor abnormalities: conflicting conceptualizations and unequal treatment
Abstract
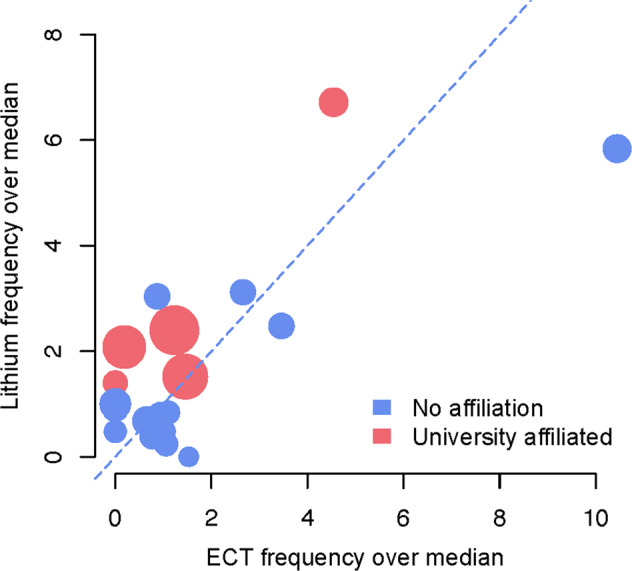
Two emerging diagnostic concepts promote distinct treatments for youth with acute-onset motor abnormalities and severe concurrent psychiatric symptoms: Pediatric acute-onset neuropsychiatric syndrome (PANS) and pediatric catatonia. Both have institutional approval in parts of Europe and in the USA, meriting an unconditional comparison of supporting evidence. Here we report results of qualitative and quantitative analyses of literature and Swedish National Registry Data suggesting that (1) catatonic patients are liable to fulfilling diagnostic criteria for PANS, (2) three conservatively assessed PANS case-reports present with possible unrecognized catatonia, (3) lithium and electroconvulsive therapy usage frequencies in Swedish minors (exclusively recommended for severe mental illness) are strongly intercorrelated and unequally distributed across Swedish counties, (4) established severe mental disorders are rarely overtly considered amongst PANS-specific research and (5) best-available evidence treatments appear markedly superior for pediatric catatonia compared to PANS in both childhood and adolescence. Prioritizing treatments for pediatric catatonia in concerned subjects could markedly improve treatment outcomes.
Keywords: Diagnosis; Paediatric research; Psychiatric disorders; Schizophrenia.
© The Author(s) 2022.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures

References
-
- Gromark C, et al. Establishing a pediatric acute-onset neuropsychiatric syndrome clinic: baseline clinical features of the pediatric acute-onset neuropsychiatric syndrome Cohort at Karolinska Institutet. J. Child Adolesc. Psychopharmacol. 2019;29:625. doi: 10.1089/cap.2018.0127. - DOI - PMC - PubMed
-
- Swedo S. E., Leckman J. F., Rose N. R. From research subgroup to clinical syndrome: modifying the PANDAS criteria to describe PANS (Pediatric Acute-onset Neuropsychiatric Syndrome). Pediatr. Ther.2. 10.4172/2161-0665.1000113 (2012).
-
- Pfeiffer HCV, et al. Clinical guidance for diagnosis and management of suspected pediatric acute-onset neuropsychiatric syndrome in the Nordic countries. Acta Paediatr. 2021;00:1–8. - PubMed
LinkOut - more resources
Full Text Sources
