

Modern Treatment of Neurogenic Thoracic Outlet Syndrome: Pathoanatomy, Diagnosis, and Arthroscopic Surgical Technique
- PMID: 37521545
- PMCID: PMC10382898
- DOI: 10.1016/j.jhsg.2022.07.004
Modern Treatment of Neurogenic Thoracic Outlet Syndrome: Pathoanatomy, Diagnosis, and Arthroscopic Surgical Technique
Abstract
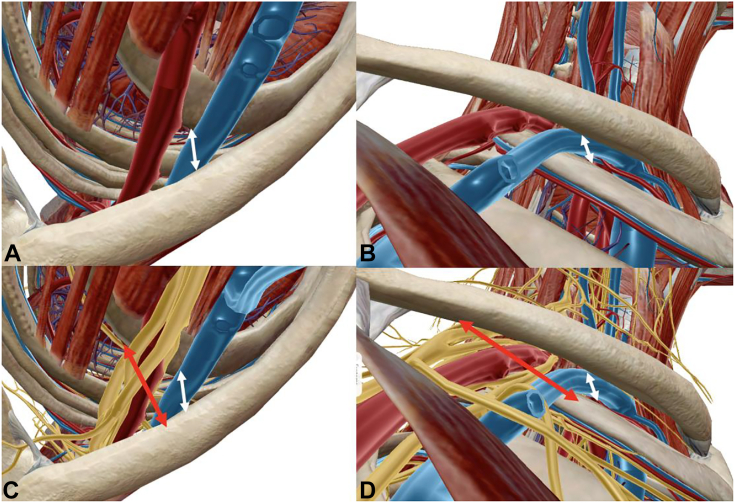
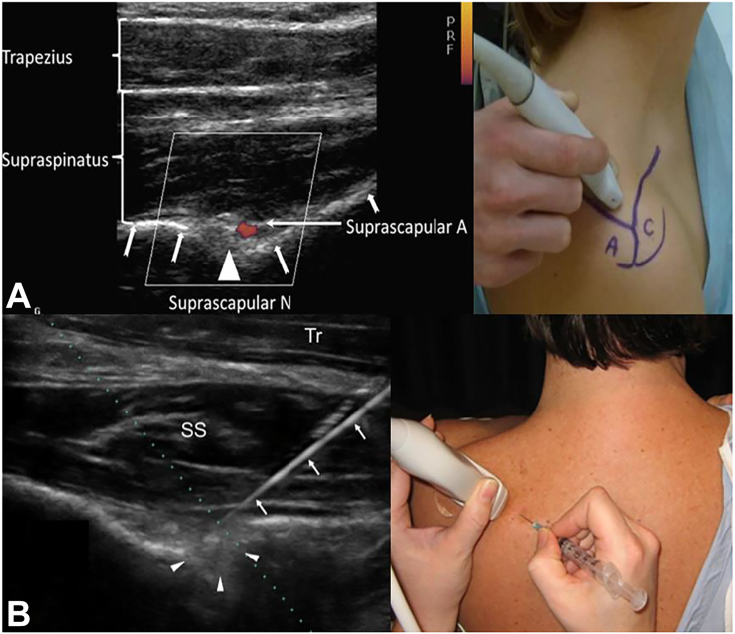
Compressive pathology in the supraclavicular and infraclavicular fossae is broadly termed "thoracic outlet syndrome," with the large majority being neurogenic in nature. These are challenging conditions for patients and physicians and require robust knowledge of thoracic outlet anatomy and scapulothoracic kinematics to elucidate neurogenic versus vascular disorders. The combination of repetitive overhead activity and scapular dyskinesia leads to contracture of the scalene muscles, subclavius, and pectoralis minor, creating a chronically distalized and protracted scapular posture. This decreases the volume of the scalene triangle, costoclavicular space, and retropectoralis minor space, with resultant compression of the brachial plexus causing neurogenic thoracic outlet syndrome. This pathologic cascade leading to neurogenic thoracic outlet syndrome is termed pectoralis minor syndrome when primary symptoms localize to the infraclavicular area. Making the correct diagnosis is challenging and requires the combination of complete history, physical examination, advanced imaging, and ultrasound-guided injections. Most patients improve with nonsurgical treatment incorporating pectoralis minor stretching and periscapular and postural retraining. Surgical decompression of the thoracic outlet is reserved for compliant patients who fail nonsurgical management and respond favorably to targeted injections. In addition to prior exclusively open procedures with supraclavicular, infraclavicular, and/or transaxillary approaches, new minimally invasive and targeted endoscopic techniques have been developed over the past decade. They involve the endoscopic release of the pectoralis minor tendon, with additional suprascapular nerve release, brachial plexus neurolysis, and subclavius and interscalene release depending on the preoperative work-up.
Keywords: Endoscopic brachial plexus neurolysis; Neurogenic thoracic outlet syndrome; Pectoralis minor release; Pectoralis minor syndrome; Suprascapular neuropathy.
© 2022 The Authors.
Figures


















References
-
- Atroshi I., Gummesson C., Johnsson R., Ornstein E., Ranstam J., Rosén I. Prevalence of carpal tunnel syndrome in a general population. JAMA. 1999;282(2):153–158. - PubMed
-
- Mondelli M., Grippo A., Mariani M., et al. Carpal tunnel syndrome and ulnar neuropathy at the elbow in floor cleaners. Neurophysiol Clin. 2006;36(4):245–253. - PubMed
-
- Kuhn J.E., Lebus V.G.F., Bible J.E. Thoracic outlet syndrome. J Am Acad Orthop Surg. 2015;23(4):222–232. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
