

National Estimates of the Adult Diabetes Care Continuum in India, 2019-2021
- PMID: 37523192
- PMCID: PMC10391358
- DOI: 10.1001/jamainternmed.2023.3070
National Estimates of the Adult Diabetes Care Continuum in India, 2019-2021
Abstract
Importance: Diabetes is widespread and treatable, but little is known about the diabetes care continuum (diagnosis, treatment, and control) in India and how it varies at the national, state, and district levels.
Objective: To estimate the adult population levels of diabetes diagnosis, treatment, and control in India at national, state, and district levels and by sociodemographic characteristics.
Design, setting, and participants: In this cross-sectional, nationally representative survey study from 2019 to 2021, adults in India from 28 states, 8 union territories, and 707 districts were surveyed for India's Fifth National Family Health Survey (NFHS-5). The survey team collected data on blood glucose among all adults (18-98 years) who were living in the same household as eligible participants (pregnant or nonpregnant female individuals aged 15-49 years and male individuals aged 15-54 years). The overall sample consisted of 1 895 287 adults. The analytic sample was restricted to those who either self-reported having diabetes or who had a valid measurement of blood glucose.
Exposures: The exposures in this survey study were district and state residence; urban vs rural residence; age (18-39 years, 40-64 years, or ≥65 years); sex; and household wealth quintile.
Main outcomes and measures: Diabetes was defined by self-report or high capillary blood glucose (fasting: ≥126 mg/dL [to convert to mmol/L, multiply by 0.0555]; nonfasting: ≥220 mg/dL). Among respondents who had previously been diagnosed with diabetes, the main outcome was the proportion treated based on self-reported medication use and the proportion controlled (fasting: blood glucose <126 mg/dL; nonfasting: ≤180 mg/dL). The findings were benchmarked against the World Health Organization (WHO) Global Diabetes Compact targets (80% diagnosis; 80% control among those diagnosed). The variance in indicators between and within states was partitioned using variance partition coefficients (VPCs).
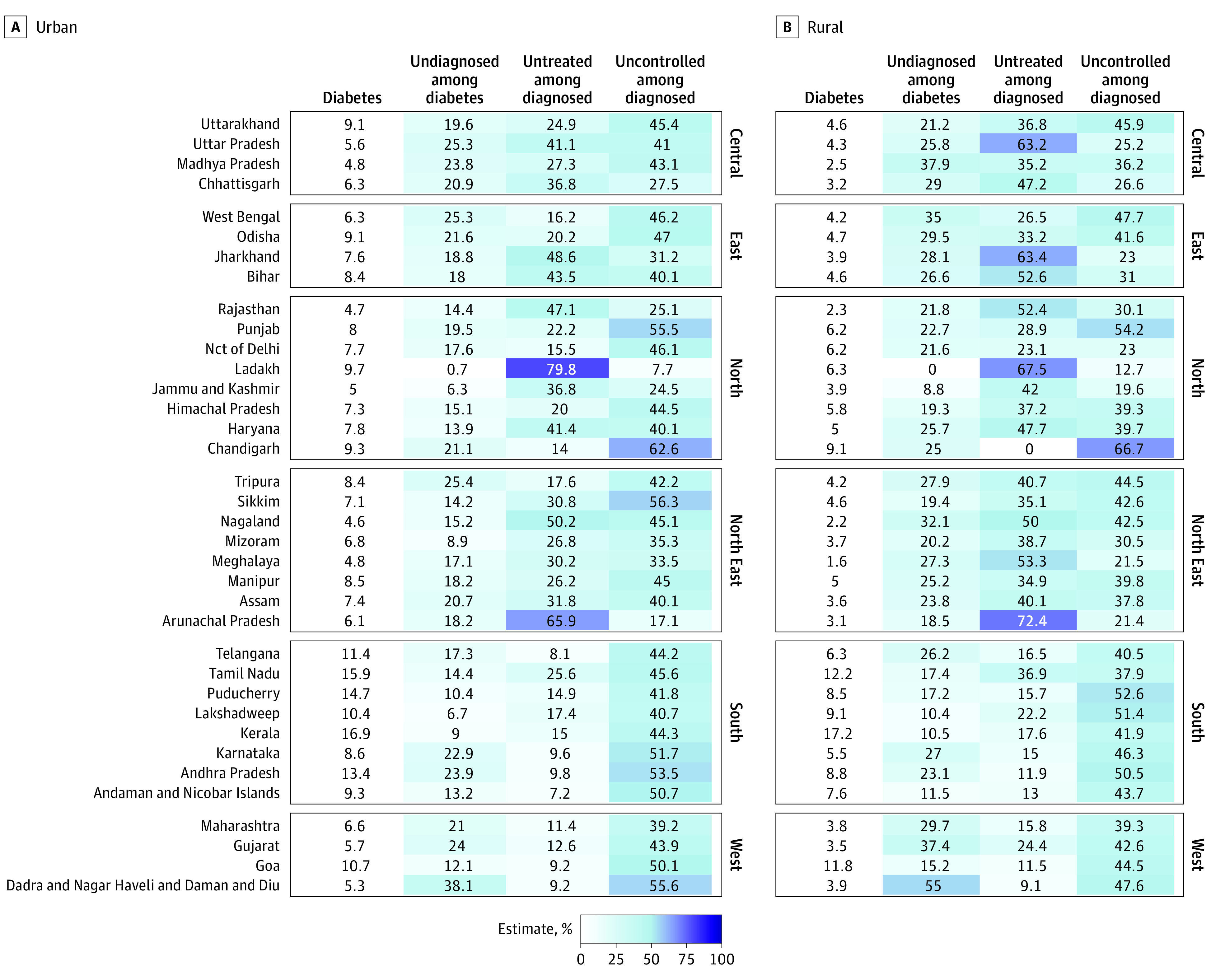
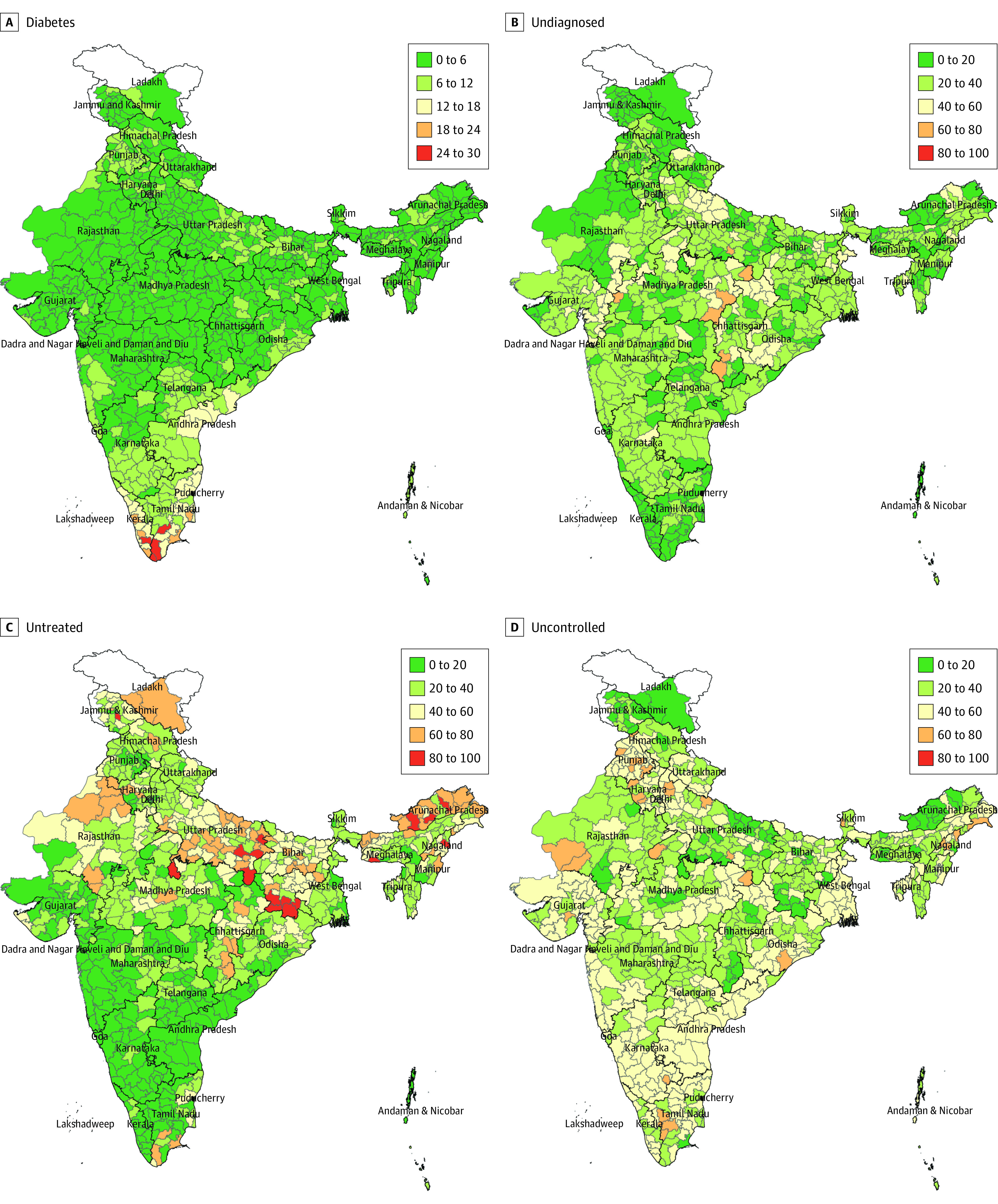
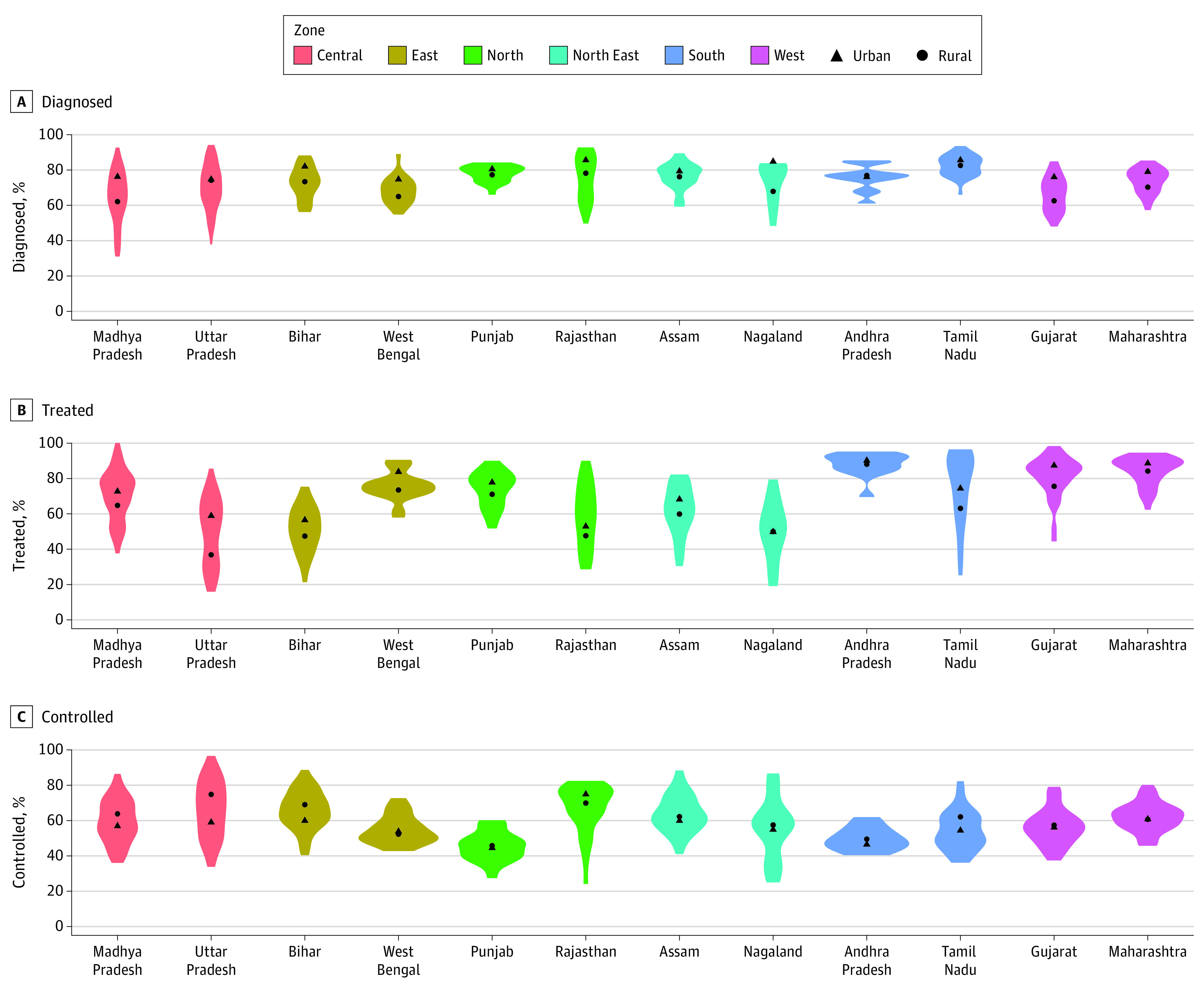
Results: Among 1 651 176 adult respondents (mean [SD] age, 41.6 [16.4] years; 867 896 [52.6%] female) with blood glucose measures, the proportion of individuals with diabetes was 6.5% (95% CI, 6.4%-6.6%). Among adults with diabetes, 74.2% (95% CI, 73.3%-75.0%) were diagnosed. Among those diagnosed, 59.4% (95% CI, 58.1%-60.6%) reported taking medication, and 65.5% (95% CI, 64.5%-66.4%) achieved control. Diagnosis and treatment were higher in urban areas, older age groups, and wealthier households. Among those diagnosed in the 707 districts surveyed, 246 (34.8%) districts met the WHO diagnosis target, while 76 (10.7%) districts met the WHO control target. Most of the variability in diabetes diagnosis (VPC, 89.1%), treatment (VPC, 85.9%), and control (VPC, 95.6%) were within states, not between states.
Conclusions and relevance: In this survey study, the diabetes care continuum in India is represented by considerable district-level variation, age-related disparities, and rural-urban differences. Surveillance at the district level can guide state health administrators to prioritize interventions and monitor achievement of global targets.
Conflict of interest statement
Figures

References
-
- International Diabetes Federation . IDF diabetes atlas. Accessed October 6, 2022. https://diabetesatlas.org/ - PubMed
-
- IDF Working Group . Adler A, Bailey C, Ascher P. IDF clinical practice recommendations for managing type 2 diabetes in primary care. 2017. Accessed August 30, 2022. https://d-net.idf.org/en/library/466-managing-type-2-diabetes-in-primary...
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
