Development and Validation of a Postprocedural Model to Predict Outcome After Endovascular Treatment for Ischemic Stroke
- PMID: 37523199
- PMCID: PMC10391355
- DOI: 10.1001/jamaneurol.2023.2392
Development and Validation of a Postprocedural Model to Predict Outcome After Endovascular Treatment for Ischemic Stroke
Abstract
Importance: Outcome prediction after endovascular treatment (EVT) for ischemic stroke is important to patients, family members, and physicians.
Objective: To develop and validate a model based on preprocedural and postprocedural characteristics to predict functional outcome for individual patients after EVT.
Design, setting, and participants: A prediction model was developed using individual patient data from 7 randomized clinical trials, performed between December 2010 and December 2014. The model was developed within the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES) collaboration and external validation in data from the Dutch Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) Registry of patients treated in clinical practice between March 2014 and November 2017. Participants included patients from multiple centers throughout different countries in Europe, North America, East Asia, and Oceania (derivation cohort), and multiple centers in the Netherlands (validation cohort). Included were adult patients with a history of ischemic stroke from an intracranial large vessel occlusion in the anterior circulation who underwent EVT within 12 hours of symptom onset or last seen well. Data were last analyzed in July 2022.
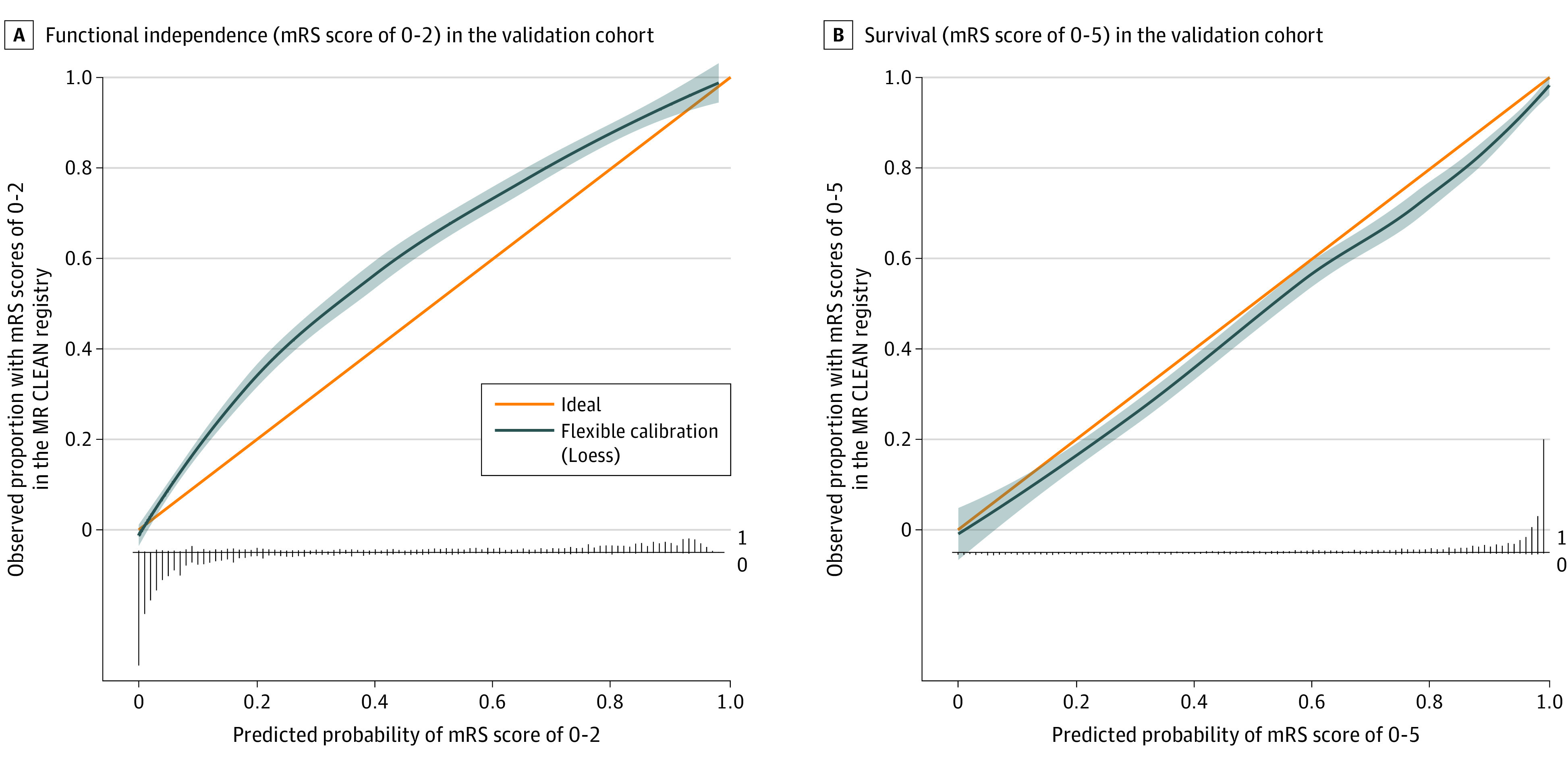
Main outcome(s) and measure(s): A total of 19 variables were assessed by multivariable ordinal regression to predict functional outcome (modified Rankin Scale [mRS] score) 90 days after EVT. Variables were routinely available 1 day after EVT. Akaike information criterion (AIC) was used to optimize model fit vs model complexity. Probabilities for functional independence (mRS 0-2) and survival (mRS 0-5) were derived from the ordinal model. Model performance was expressed with discrimination (C statistic) and calibration.
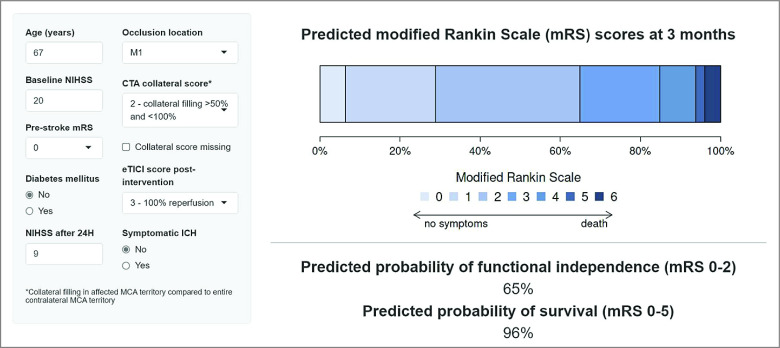
Results: A total of 781 patients (median [IQR] age, 67 [57-76] years; 414 men [53%]) constituted the derivation cohort, and 3260 patients (median [IQR] age, 72 [61-80] years; 1684 men [52%]) composed the validation cohort. Nine variables were included in the model: age, baseline National Institutes of Health Stroke Scale (NIHSS) score, prestroke mRS score, history of diabetes, occlusion location, collateral score, reperfusion grade, NIHSS score at 24 hours, and symptomatic intracranial hemorrhage 24 hours after EVT. External validation in the MR CLEAN Registry showed excellent discriminative ability for functional independence (C statistic, 0.91; 95% CI, 0.90-0.92) and survival (0.89; 95% CI, 0.88-0.90). The proportion of functional independence in the MR CLEAN Registry was systematically higher than predicted by the model (41% vs 34%), whereas observed and predicted survival were similar (72% vs 75%). The model was updated and implemented for clinical use.
Conclusion and relevance: The prognostic tool MR PREDICTS@24H can be applied 1 day after EVT to accurately predict functional outcome for individual patients at 90 days and to provide reliable outcome expectations and personalize follow-up and rehabilitation plans. It will need further validation and updating for contemporary patients.
Conflict of interest statement
Figures