

A Polygenic Risk Score for Idiopathic Pulmonary Fibrosis and Interstitial Lung Abnormalities
- PMID: 37523715
- PMCID: PMC10563194
- DOI: 10.1164/rccm.202212-2257OC
A Polygenic Risk Score for Idiopathic Pulmonary Fibrosis and Interstitial Lung Abnormalities
Erratum in
-
Erratum: A Polygenic Risk Score for Idiopathic Pulmonary Fibrosis and Interstitial Lung Abnormalities.Am J Respir Crit Care Med. 2024 Apr 15;209(8):1045. doi: 10.1164/rccm.v209erratum5. Am J Respir Crit Care Med. 2024. PMID: 38619438 Free PMC article. No abstract available.
Abstract
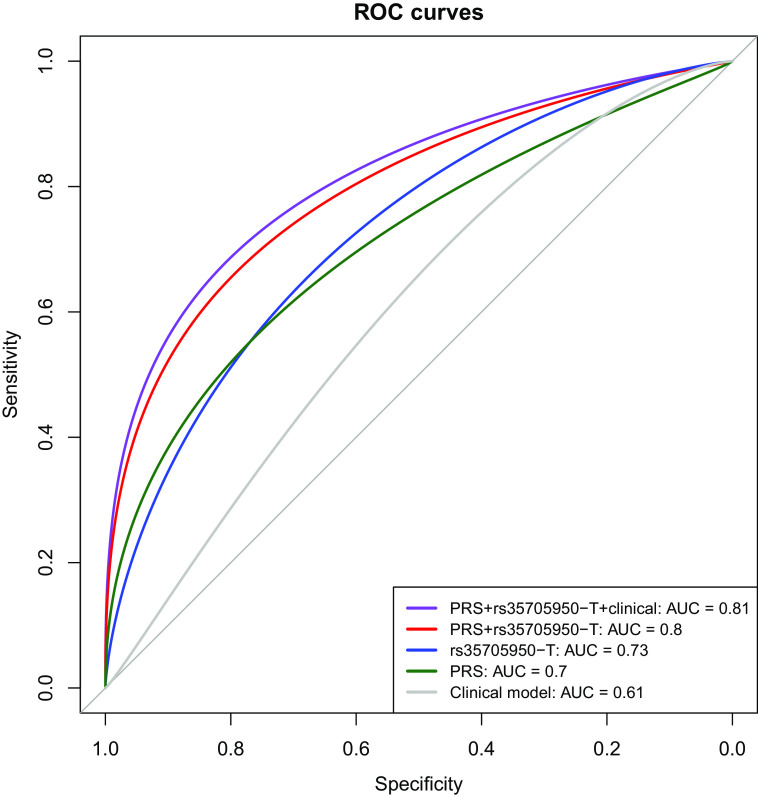
Rationale: In addition to rare genetic variants and the MUC5B locus, common genetic variants contribute to idiopathic pulmonary fibrosis (IPF) risk. The predictive power of common variants outside the MUC5B locus for IPF and interstitial lung abnormalities (ILAs) is unknown. Objectives: We tested the predictive value of IPF polygenic risk scores (PRSs) with and without the MUC5B region on IPF, ILA, and ILA progression. Methods: We developed PRSs that included (PRS-M5B) and excluded (PRS-NO-M5B) the MUC5B region (500-kb window around rs35705950-T) using an IPF genome-wide association study. We assessed PRS associations with area under the receiver operating characteristic curve (AUC) metrics for IPF, ILA, and ILA progression. Measurements and Main Results: We included 14,650 participants (1,970 IPF; 1,068 ILA) from six multi-ancestry population-based and case-control cohorts. In cases excluded from genome-wide association study, the PRS-M5B (odds ratio [OR] per SD of the score, 3.1; P = 7.1 × 10-95) and PRS-NO-M5B (OR per SD, 2.8; P = 2.5 × 10-87) were associated with IPF. Participants in the top PRS-NO-M5B quintile had ∼sevenfold odds for IPF compared with those in the first quintile. A clinical model predicted IPF (AUC, 0.61); rs35705950-T and PRS-NO-M5B demonstrated higher AUCs (0.73 and 0.7, respectively), and adding both genetic predictors to a clinical model yielded the highest performance (AUC, 0.81). The PRS-NO-M5B was associated with ILA (OR, 1.25) and ILA progression (OR, 1.16) in European ancestry participants. Conclusions: A common genetic variant risk score complements the MUC5B variant to identify individuals at high risk of interstitial lung abnormalities and pulmonary fibrosis.
Keywords: MUC5B; idiopathic pulmonary fibrosis; interstitial lung abnormalities; polygenic risk score.
Figures



Comment in
-
PRS-ing Forward to Identify Genetic Risk in Idiopathic Pulmonary Fibrosis.Am J Respir Crit Care Med. 2023 Oct 1;208(7):750-752. doi: 10.1164/rccm.202308-1373ED. Am J Respir Crit Care Med. 2023. PMID: 37607347 Free PMC article. No abstract available.
References
-
- Lederer DJ, Martinez FJ. Idiopathic pulmonary fibrosis. N Engl J Med . 2018;378:1811–1823. - PubMed
-
- Raghu G, Chen SY, Yeh WS, Maroni B, Li Q, Lee YC, et al. Idiopathic pulmonary fibrosis in US Medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001-11. Lancet Respir Med . 2014;2:566–572. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL152728/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- R01 HL133135/HL/NHLBI NIH HHS/United States
- P30 DK063491/DK/NIDDK NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268200900018C/HL/NHLBI NIH HHS/United States
- HHSN268200900017C/HL/NHLBI NIH HHS/United States
- P01 HL132825/HL/NHLBI NIH HHS/United States
- P01 HL114501/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- HHSN268200900019C/HL/NHLBI NIH HHS/United States
- P01 HL092870/HL/NHLBI NIH HHS/United States
- R01 AR077607/AR/NIAMS NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- R01 HL120393/HL/NHLBI NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N02 HL064278/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- P30 AR072577/AR/NIAMS NIH HHS/United States
- R01 HL155522/HL/NHLBI NIH HHS/United States
- R01 HL158668/HL/NHLBI NIH HHS/United States
- R01 HL130974/HL/NHLBI NIH HHS/United States
- U01 HL120393/HL/NHLBI NIH HHS/United States
- R01 HL153248/HL/NHLBI NIH HHS/United States
- U01 HL089897/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- UH3 HL151865/HL/NHLBI NIH HHS/United States
- DH_/Department of Health/United Kingdom
- R01 HL111527/HL/NHLBI NIH HHS/United States
- P30 AR070253/AR/NIAMS NIH HHS/United States
- RC1 HL100543/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- K01 HL157613/HL/NHLBI NIH HHS/United States
- R01 HL147148/HL/NHLBI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- R01 AR080659/AR/NIAMS NIH HHS/United States
- T32 AR007530/AR/NIAMS NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- HHSN268201000021C/HL/NHLBI NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- N02 HL64278/HL/NHLBI NIH HHS/United States
- R01 HL111024/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- HHSN268200900015C/HL/NHLBI NIH HHS/United States
- HHSN268200900016C/HL/NHLBI NIH HHS/United States
- R01 HL135142/HL/NHLBI NIH HHS/United States
- I01 BX005295/BX/BLRD VA/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- R01 HL121270/HL/NHLBI NIH HHS/United States
- U01 HL137880/HL/NHLBI NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- K08 HL159318/HL/NHLBI NIH HHS/United States
- R01 HL137927/HL/NHLBI NIH HHS/United States
- K08 HL136928/HL/NHLBI NIH HHS/United States
- R01 HL142992/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- 75N92019D00031/HL/NHLBI NIH HHS/United States
- HHSN268200900013C/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- N01 HC095166/HL/NHLBI NIH HHS/United States
- UG3 HL151865/HL/NHLBI NIH HHS/United States
- R01 CA203636/CA/NCI NIH HHS/United States
- P01 HL162607/HL/NHLBI NIH HHS/United States
- K23 HL150301/HL/NHLBI NIH HHS/United States
- U01 CA209414/CA/NCI NIH HHS/United States
- R01 HL117626/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- HHSN268200900014C/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- R01 HL149836/HL/NHLBI NIH HHS/United States
- T32 HL007427/HL/NHLBI NIH HHS/United States
- HHSN268201000001I/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
