

Rationale and design of an investigator-initiated, multicenter, prospective, placebo-controlled, double-blind, randomized trial to evaluate the effects of finerenone on vascular stiffness and cardiorenal biomarkers in type 2 diabetes and chronic kidney disease (FIVE-STAR)
- PMID: 37525257
- PMCID: PMC10391880
- DOI: 10.1186/s12933-023-01928-y
Rationale and design of an investigator-initiated, multicenter, prospective, placebo-controlled, double-blind, randomized trial to evaluate the effects of finerenone on vascular stiffness and cardiorenal biomarkers in type 2 diabetes and chronic kidney disease (FIVE-STAR)
Abstract
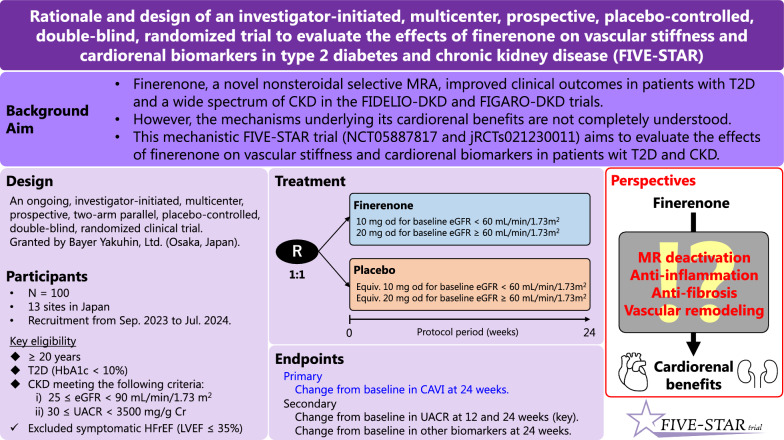
Background: The overactivation of mineralocorticoid receptor (MR) plays a key pathological role in the progression of cardiovascular and renal diseases by promoting pro-inflammatory and pro-fibrotic signaling. Recently, it has been found that finerenone, a novel nonsteroidal selective MR antagonist, can robustly improve cardiorenal outcomes in patients with type 2 diabetes (T2D) and a wide spectrum of chronic kidney disease (CKD). However, the mechanisms underlying the cardiorenal benefits of finerenone are poorly understood. Further, whether the clinical benefits are mediated by an improvement in vascular stiffness is not confirmed. Therefore, the current study aims to evaluate the effects of finerenone on vascular stiffness as assessed using cardio ankle vascular index (CAVI) and relevant cardiorenal biomarkers in patients with T2D and CKD.
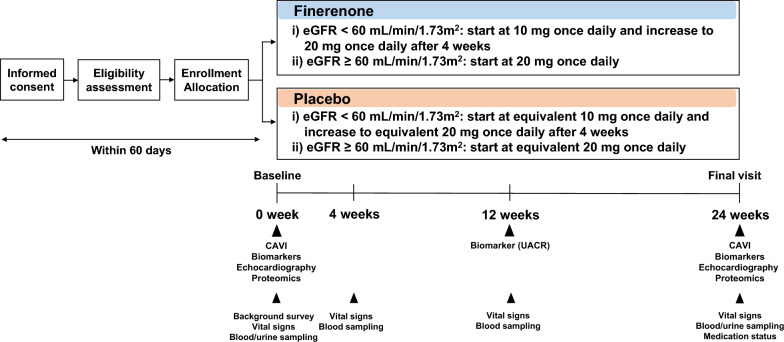
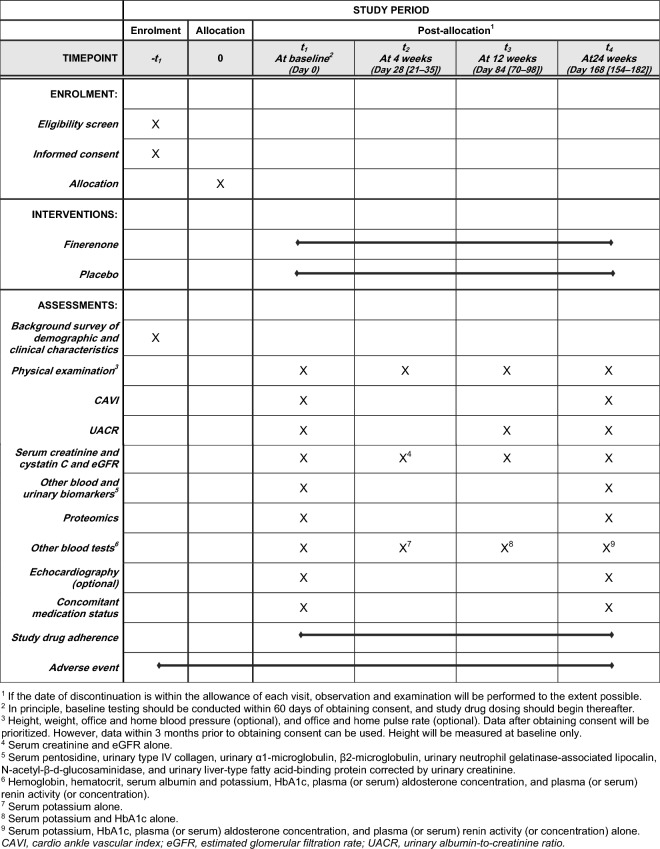
Methods: The Effects of Finerenone on Vascular Stiffness and Cardiorenal Biomarkers in Type 2 Diabetes and Chronic Kidney Disease (FIVE-STAR) is an ongoing, investigator-initiated, multicenter, prospective, placebo-controlled, double-blind, randomized clinical trial in Japan. Its target sample size is 100 subjects. Recruitment will be performed from September 2023 to July 2024. After obtaining informed consent, eligible participants with T2D and CKD (25 mL/min/1.73 m2 ≤ estimated glomerular filtration ratio [eGFR] < 90 mL/min/1.73 m2 and 30 mg/g Cr ≤ urinary albumin-to-creatinine ratio [UACR] < 3500 mg/g Cr) will be equally randomized to receive 24-week treatment with either finerenone (starting dose at 10 mg once daily in participants with a baseline eGFR < 60 mL/min/1.73 m2 or at 20 mg once daily in those with a baseline eGFR ≥ 60 mL/min/1.73 m2) or dose-matched placebo. The primary endpoint is the change from baseline in CAVI at 24 weeks. The secondary endpoints are changes from baseline in UACR at 12 and 24 weeks and relevant serum and urinary biomarkers at 24 weeks. As an exploratory endpoint, proteomic analysis using the Olink® Target 96 panels will be also performed.
Discussion: FIVE-STAR is the first trial evaluating the therapeutic impact of finerenone on vascular stiffness and relevant cardiorenal biomarkers in patients with T2D and CKD. This study will provide mechanistic insights on the clinical benefits of finerenone based on recent cardiovascular and renal outcome trials. Trial registration Unique Trial Number, NCT05887817 ( https://clinicaltrials.gov/ct2/show/NCT05887817 ) and jRCTs021230011 ( https://jrct.niph.go.jp/latest-detail/jRCTs021230011 ).
Keywords: Biomarker; Chronic kidney disease; Finerenone; Type 2 diabetes; Vascular stiffness.
© 2023. The Author(s).
Conflict of interest statement
AT received honoraria from Boehringer Ingelheim and research funding from GlaxoSmithKline, Takeda, Bristol-Myers Squibb and Novo Nordisk. HS has received speaking fees from Bayer, Daiichi Sankyo, AstraZeneca, and Novartis Pharma and scholarship from Bayer and Chugai Pharmaceutical. TI received lecture fees from JCR Pharmaceuticals and Kyowa Kirin. HY reported receiving lecture fee from Kyowa Kirin. MMiyazono has received honoraria from Chugai Pharmaceutical, Astellas, Kyowa Kirin, Mitsubishi Tanabe, Mochida Pharmaceutical, AstraZeneca, Bayer Yakuhin, Torii Pharmaceutical, Fuso Pharmaceutical Industries, Teijin Pharma, and Kissei Pharmaceutical, research grant from Chugai Pharmaceutical, and scholarship from Kyowa Kirin, Torii Pharmaceutical, Fuso Pharmaceutical Industries, and Kissei Pharmaceutical. NT received honoraria from Daiichi Sankyo, Novartis Pharma, Boehringer Ingelheim, Toa Eiyo, Bristol Myers Squibb, Pfizer, AstraZeneca, and Bayer Yakuhin. DF has received honoraria from Bayer Yakuhin, Daiichi Sankyo, and Otsuka Pharmaceutical. HT received research grants from AstraZeneca, Daiichi Sankyo, Janssen, Novo Nordisk, and Eli Lilly. KK received honoraria from AstraZeneca, Ono Pharmaceutical, Boehringer Ingelheim, Otsuka Pharmaceutical, and Novartis Pharma. MMoroi has received honoraria from Takeda, Sanofi, Bayer, Otsuka Pharmaceutical, Mitsubishi Tanabe, and Amicus Therapeutics and research grant from Teijin Pharma, Sanofi, Nihon Medi-physics, and Amicus Therapeutics. ST received honoraria from Otsuka Pharmaceutical, Ono Pharmaceutical, Daiichi Sankyo, Bayer Yakuhin, AstraZeneca, and Novartis Pharma. MS has received speaker's honoraria from Bayer Yakuhin. KT has received honoraria from Abbott Medical, Boston Scientific, Orbusneich, Kaneka, Japan Lifeline, Edwards Lifesciences, HeatFlow, Bayer Yakuhin, Medis, and Daiichi Sankyo. MN has received lecture fees from Kyowa Kirin, Astellas, GlaxoSmithKline, Daiichi Sankyo, Mitsubishi Tanabe, Chugai Pharmaceutical, Torii Pharmaceutical, JT, Alexion, Akebia, MSD, and Boehringer Ingelheim and research support from JT, Kyowa Kirin, Astellas, Ono Pharmaceutical, Takeda, Daiichi Sankyo, Mitsubishi Tanabe, Chugai Pharmaceutical, Torii Pharmaceutical, Kissei Pharmaceutical, and Boehringer Ingelheim. KN has received honoraria from AstraZeneca, Bayer Yakuhin, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly Japan, Kowa, Mitsubishi Tanabe, MSD, Novartis Pharma, Novo Nordisk, Ono Pharmaceutical, Otsuka Pharmaceutical, and Takeda, research grant from Asahi Kasei, Astellas, Boehringer Ingelheim, Fuji Yakuhin, Mitsubishi Tanabe, Mochida Pharmaceutical, Novartis Pharma, and Teijin Pharma, and Scholarship from Bayer Yakuhin, Medtronic, Teijin Pharma. AT and KN are Editorial Board members of the journal, and they were not involved in handling this manuscript during the submission and the review processes. Other authors declare no potential conflict of interest.
Figures
References
-
- de Boer IH, Khunti K, Sadusky T, Tuttle KR, Neumiller JJ, Rhee CM, Rosas SE, Rossing P, Bakris G. Diabetes management in chronic kidney disease: a consensus report by the American diabetes association (ADA) and kidney disease: improving global outcomes (KDIGO) Kidney Int. 2022;102(5):974–989. doi: 10.1016/j.kint.2022.08.012. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
